




Survivability Drift Theory and Attrition Mitigation in Special Operations Forces


Abstract
Survivability Drift Theory (SDT) provides a practical framework to interrupt escalating attrition in special operations forces (SOF). Despite elite selection and resilience-focused programming, negative survivability trends in SOF account for losses that in other warfighting systems would trigger invasive corrective action. SDT identifies these patterned losses not as random, but as a progressive, detectable syndrome—drift, that unfolds across six key domains: neurological, moral, relational, cognitive, interoceptive, and identity. Drift is recursive, measurable, and reversible, providing commanders and clinicians with actionable opportunities for intervention before catastrophic endpoints.
Survivability, under this model, is no longer a binary (life or death) but a dynamic, longitudinal capacity affected by cumulative exposures: blast injury, role erosion, and combat exposures, among others. Rather than replacing clinical autonomy, SDT equips leadership with a surveillance lens and operational vocabulary for force health protection. The theory underpins novel SOF-specific clinical and diagnostic methods now in development, enabling units to track drift markers and force-level trends. Adoption of SDT principles can better enable commanders across SOF to steer survivability trajectories and mitigate attrition to better preserve this strategic national asset.
Introduction and Theoretical Context
Special operations forces worldwide remain high-performance ecosystems—bearing the brunt of two decades of counterterrorism operations while shifting to the demands of strategic competition today. (See Note 1). Despite the abundance of resilience-focused programming and various U.S. military wellness efforts, too many Operators have perished from attrition: dying by suicide or, at minimum, abruptly departing roles or teams for which they and their families have sacrificed so much. (See Notes 1-7).
Special Operators remain highly resilient and mission-critical tacticians, yet despite their elite selection and entrenched invincibility, suicide incidence in GWOT-era American SOF reveals a reversed survivability trend in attrition. (See Notes 1-3). Current prevalence-based comparisons, such as suicides per 100,000, drastically underestimate risk in SOF by failing to account for multiple variables like op tempo, kinetic density, and cumulative physiologic derangement. At present, even our cursory calculations of fatality data also found Operator suicide risk averaged to 75% higher than conventional U.S. military forces, supported by suicide accounting for 1 in every 33 SOF fatalities in Iraq theaters and 1 in every 100 SOF deployment deaths across all combatant commands. (See Note 1).
In any other high-value operational system, a 3% loss to a single failure mode would be considered catastrophic, declared non-mission-capable, and subjected to immediate institutional review and corrective action. Suicides occurring in a force engineered for resilience and survival warrants no less doctrinal and operational urgency. The core issue lies not within ratios and prevalence counts, but in degraded survivability manifesting within a specifically selected population in which every loss is a strategic national asset.
These events, especially within an exceptionally resilient ecosystem, appear to represent a progressive, detectable syndrome rather than an unpredictable or individualized phenomenon. We therefore propose Survivability Drift Theory (SDT) as a framework to guide clinical, operational, and policy interventions in high-risk SOF populations. Key aspects of SDT span the neurological, moral, relational, cognitive, interoceptive, and identity domains. Though originally conceptualized for special mission units, SDT’s cross-cutting explanatory value across the entire SOF enterprise quickly became apparent during theory construction.
Not designed to replace clinicians’ autonomy or medical diagnostics, SDT instead serves to surveil and flag early warning signs in direct-action SOF and special mission personnel under cumulative exposure conditions (blast-overpressure, institutional tension, hazardous materials, role erosion), and may generalize to other high-risk populations (e.g., first responders, intelligence operatives, etc.). (See Notes 1, 3, 8, 9).
Background and Theoretical Roots
Survivability drift in SDT is akin to tactical driving drift: cumulative forces—if not detected and corrected early—cause progressive loss of control. Just as skilled drivers learn to recognize early vehicle drift and adjust inputs before catastrophic loss, SDT emphasizes Operator-centered surveillance to detect survivability drift before irreversible collapse.
Based on our combined SOF-centric studies and efforts, SDT addresses a persistent conceptual gap: clinicians are typically presented with survivability as a binary concept (life vs. death, broken vs. not broken), yet we argue most SOF attrition arises through gradual degradation—not a single driving catastrophic event. (See Notes 1, 3, 8-52). Drawing from gold-standard theory construction models, we relate here a repeatedly observed condition in SOF that remains unnamed: a drift away from survivability. (See Notes 53-57).
We redefine SOF survivability as a multidimensional capacity rather than a terminal outcome, building on the evolutionary concept analysis methodology used previously to redefine SOF-situated trauma and resilience. (See Notes 58, 52, and 46). Though credible interpersonal theories certainly explain important elements of suicidality in Special Operations, SDT has a broader umbrella under which we reposition survivability as a situated, longitudinal construct influenced by both institutional-operational exposures and individual identity coherence.
Drift, however, is the central phenomenon—the progressive, syndromic loss of survivability across neurological, moral, relational, cognitive, interoceptive, and identity domains. It is patterned, cumulative, measurable, and reversible. Losses in Operator function within those domains explains eventual disengagement, physical collapse, and suicide. Drift is neither an abstraction nor metaphor—it is a real, lived, and empirically observable trajectory.
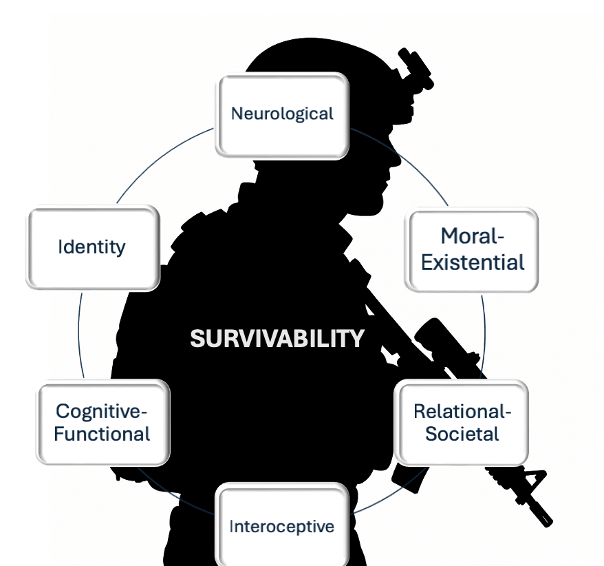
Figure 1. Visual model of SDT domains.
Assumptions:
- Survivability exists on a continuum and is not a dichotomous outcome.
- Survivability loss is detectable before catastrophic endpoints.
- Institutions share responsibility for drift detection and prevention.
- Survivability degradation is not suboptimal resilience nor a behavioral response.
- Survivability reflects physiological, relational, and moral collapse.
Theoretical Key Components: Survivability and Drift
As apparent in SDT’s title, survivability and drift comprise the key components of the theory. Survivability refers to an operator’s ability to maintain whole-person functioning across their entire service arc and into post-service life. It is determined by whether the operator remains coherent and adaptive across six domains: neurological, moral, relational,cognitive, interoceptive (body-state), and identity.
In simple terms, can the Operator still think clearly, feel purpose, stay connected to/lead others, read their own body accurately, and retain a stable sense of self—even after cumulative operational exposures? For example, an Operator with years of blast exposure who is still sleeping well, thinking clearly, maintaining family bonds, and feeling purposeful—even with medical support, is demonstrating sustained survivability and readiness. Likewise, an operator who is post-retirement but remains engaged with their community and stable in health is also surviving well across domains.
Drift refers to the gradual, subclinical erosion of survivability—a process that builds slowly and silently, until critical collapse. Drift accumulates when exposures and injuries (such as blast overpressure, moral injury, physiological strain, survivor’s guilt, chronic injuries, family fracturing) begin to undermine domain integrity. This degradation loops recursively, weakening multiple domains simultaneously until survivability is threatened to the point where attrition is likely.
In simple terms, excessive exposure to blast overpressure, chronic insomnia and neuro-muscular pain leads to rage, ensuing shame, and cognitive fog, which in turn erodes identity and increases family strain—driving isolation and further body dysregulation until the whole system drifts toward collapse unless interrupted. For example, an Operator who can no longer regulate anger, cannot sleep through the night, forgets tasks, avoids family, loses confidence, and starts showing unexplained health problems is in active survivability drift, even if they are still technically cleared to deploy. Indeed, an Operator in drift is not “good to go.”
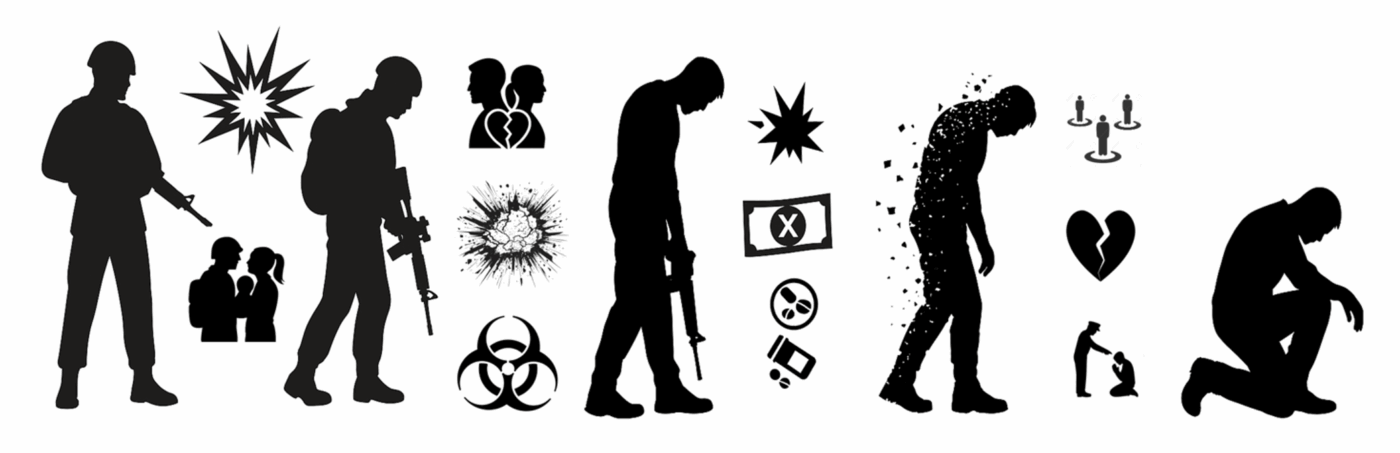
Figure 2. Visual model of unmitigated Survivability Drift: Operator Exposures (e.g., repetitive blasts, family separations, hazards) → Domain degradation → Drift (e.g., physical, family, financial) → Drift Accumulation (e.g., burdensomeness, isolation, discipline) → Collapse
The domains of drift include:
- Neurological: unprovoked irritation, unrelenting pain, disrupted sleep, impaired coordination, emergent addiction, sensory changes (vision, hearing, smell, taste, touch, etc.), unreasonable paranoia;
- Moral-Existential: self-concealment, resentment, loss of purpose, betrayal, value conflicts, trauma, disillusionment, frustrated perfectionism, uncharacteristic dishonesty;
- Relational-Societal: empathy decay, breakups, emotional blunting, legal exposures (divorce/custody), rejecting norms, financial difficulties, family disintegration, self-imposed isolation;
- Interoceptive: inexplicable fatigue, hormonal/metabolic, inflammation, autonomic instability, chronic conditions, weight fluctuation;
- Cognitive-Functional: unusual decision-making, marked avoidance, memory gaps, inattentiveness, executive dysfunction, procedural slips, masked degradation; and
- Identity: “going quiet,” persona creation, hyper- or hypo-deployable, fractured operational self, detachment from future, vocational despair, collapse of self-concept.
| SDT Domain | Functional / Stable | Emerging Drift | Advanced Drift | Catastrophic |
| Neurological | Normal sleep, no pain | Disrupted sleep, headaches | Chronic pain, sensory changes, irritability | Coordination loss, emergent addiction |
| Moral-Existential | Purpose-driven, aligned | Frustration, subtle withdrawal | Resentment, self-concealment | Value collapse, suicidal ideation |
| Relational-Societal | Strong unit/family ties | Withdrawing from friends | Family strain, legal conflicts | Isolation, divorce, estrangement |
| Interoceptive | Stable energy, metabolic balance | Fatigue, minor weight changes | Chronic fatigue, inflammatory conditions | Systemic illness, collapse |
| Cognitive-Functional | Sharp, adaptive | Memory gaps, decision fatigue | Executive dysfunction, errors | Task failure, operational removal |
| Identity | Coherent, mission-driven | Increased masking, detachment | “Going quiet,” fractured self | Total identity collapse, suicide |
Table 1. Domains of drift.
Of note, drift in one domain heightens vulnerability in others, creating a powerful positive feedback loop. Core assertions include:
- Drift is recursive, progressive, and syndromic.
- Drift is reversible, if caught early.
- Failure to intervene is institutional neglect.
- Operators rarely drift alone or without witnesses.
- Systems induce or permit the conditions.
Usefulness, Testability, and Contribution to Knowledge
Usefulness. Survivability Drift Theory scaffolds the framework for symptom quantification, targeted precision medicine, survivability interventions, and informs doctrinal reform. It does this specifically by naming and structuring survivability erosion patterns seen in SOF populations and providing diagnostic and operational vocabulary for recognizing and interrupting these trajectories.
Testability. We are testing SDT through instrument analyses and planned comparisons to physiological and biomarker data in follow-on studies. Psychometric testing of the Froede-Larkin Assessment of Repetitive Exposures in SOF scale (FLARES; developed by authors KR and JMB, with Operators, to capture subtle drift) shows promising operational utility and initial theory confirmation. (See Note 44). It is a stable 36-item scale designed to quantify subclinical drift for clinicians and commanders across domains. Criteria embedded in Combat-Related Overpressure Wave Neurotrauma and Sequelae (CROWNS), also developed with Operator input, formally classifies drift as a syndrome and generates from FLARES outputs and SDT domains (explained further in adjacent manuscripts). (See Note 42).
Given that Operators are historically opposite to malingerers (e.g., SOF are far more likely to conceal injuries or deny suffering than disclose), FLARES incorporates statistical design to detect masking and downplay of symptoms and is structured for recurrent and modular use across SOF operational timelines, to feed into a digital command dashboard for aggregate readiness and force strength estimations. (See Notes 1, 42, 44).
Contribution. This theory reframes suicide and attrition as syndromic versus surprising, and bridges clinical, operational, and doctrinal silos. To our knowledge, this is the first Operator-centered theoretical framework to address SOF-specific exposure outcomes, while providing actionable metrics for command and leadership via an integrated survivability model to inform screening, intervention, and accountability systems.
Correcting Operator Drift—Steer into the Slide, Control the Drift Angle
In the tactical driving frame, the brain functions as the engine control system—governing not only cognitive steering, but physiological traction and relational stability. Survivability is the whole drive system: body, relationships, cognition, identity—all connected. When drift sets in, it is analogous to throwing the vehicle into a slide on black ice. Skill helps, but if you miss the early signals, recovery gets exponentially harder. Likewise, functional degradation via repeated blast exposures, moral injury, and/or accumulated physiological stress is like progressive loss of traction: the Operator still moves, but is increasingly off-line, harder to stabilize, and burning out unseen systems, regardless of their resilience.
| Tactical Driving Drift | SDT Survivability Drift |
| Vehicle drifts off intended path | Operator drifts off survivability domain trajectory |
| Small uncorrected inputs accumulate | Subclinical domain erosion accumulates |
| Lateral forces magnify if unaddressed | Domain interactions amplify degradation |
| Delayed correction = harder recovery | Late intervention = harder to reverse drift |
| Skilled drivers detect early and adjust | Surveillance detects early drift, enables reversal |
Table 2. Survivability drift compared to tactical driving.
Survivability drift is not a failure of the driver—it is the product of when too many internal systems redline or misfire under unchecked demand and persistent load. Just as a skilled driver cannot override a failing traction system forever, even elite Operators will crash out without deliberate upstream monitoring and adjustment of system integrity.
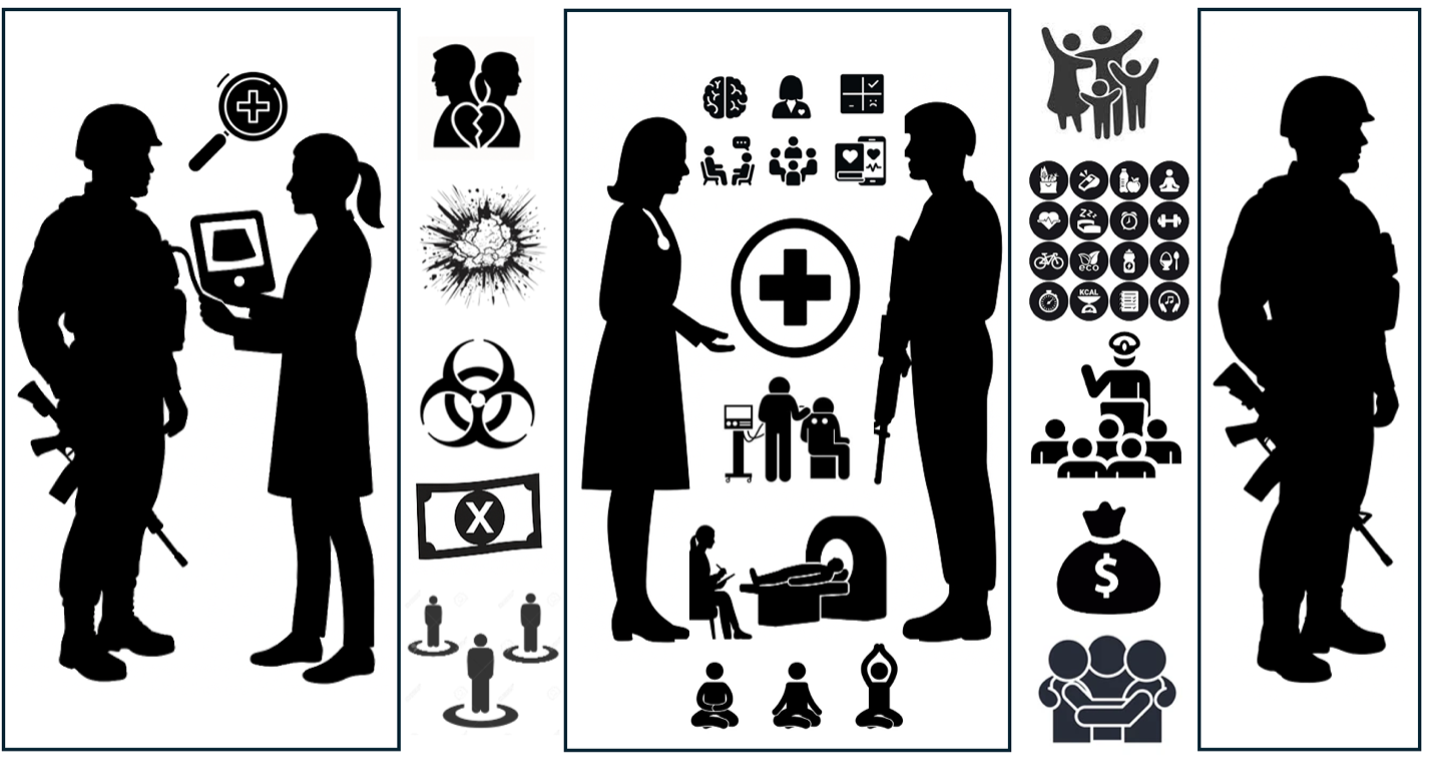
Figure 3. Visual model of mitigated drift: Targeted surveillance of domains → exposures and drifting captured → multi-disciplinary interventions launched → reassessment → restoration of function (e.g., family, health, leadership ability, force strength, financial, social reengagement).
Looking to the Future of SOF Cognitive Resilience
We grounded Survivability Drift Theory in SOF realities and experiences for institutional application. It reshapes SOF survivability as an upstream and measurable trajectory rather than a regrettable departure or postmortem summary. By offering quantification and up-front detection, the SDT framework holds potential to reduce operator suicides and reorient force health protection while providing actionable clinical intelligence for command intervention. Future steps include multinational FLARES testing, implementation, and refinement; diagnostic criteria and disease classification for CROWNS; and doctrinal integration across SOCOM (e.g., Preservation of the Force and Family [POTFF]) and NATO-aligned medical and readiness system. (See Notes 1, 44). We know blast trauma progresses as Operators’ brains and bodies age, and suicides continue to plague the SOF community. This is important now more than ever, not only impacting the families of those involved, but also reducing a critical, outsized capability necessary to achieve U.S. national security interests against both state and non-state adversaries.
Notes:
(1) Rocklein, K., Paun, O., Hamilton, R., Shattell, M., Held, P., Chandler, G., & Viola, S. (2025). No Sky Too High, No Sea Too Rough: Qualitative Investigation of Resilience and Suicide in Special Operations Forces Service Members. Journal of Psychosocial Nursing and Mental Health Services, 63(5), 26-38.
(2) Government Accountability Office. (2023, April 27). Special operations forces: Actions needed to assess performance of the Preservation of the Force and Family Program (GAO-23-105644). https://www.gao.gov/assets/gao-23-105644.pdf
(3) Rocklein Kemplin, K., Paun, O., Godbee, D., Brandon, J. (2019). Resilience and suicide in Special Operations Forces: State of the science via integrative review. The Journal of Special Operations Medicine, 19(2), 57-66.
(4) Starr, B. (2019a, February 2). US Special Ops suicides triple in 2018, as military confronts the issue. CNN. https://www.cnn.com/2019/02/02/politics/socom-military-suicide-spike-2018/index.html
(5) Starr, B. (2019b, September 26). Military Suicides Continue to Rise. CNN. https://www.cnn.com/2019/09/26/politics/military-suicides-rise/index.html
(6) Altman, H. (2017, May 13). Altman column: Suicide rate for commandos continues to decline. Tampa Bay Times. https://www.tampabay.com/news/military/macdill/altman-column-suicide-rate-for-commandos-continues-to-decline/2323420/
(7) Zoroya, G. (2013, 9 July). Special forces’ marriages on shaky ground, survey shows. USA TODAY. https://www.usatoday.com/story/news/nation/2013/07/09/marriages-military-families-elite-troops-stress/2432243
(8) Moceri-Brooks, J., Garand, L., Sekula, L. K., & Joiner, T. E. (2024a). Exploring the use of the Interpersonal Needs Questionnaire to examine suicidal thoughts and behaviors among Post-9/11 US Combat Veterans: An integrative review. Military Psychology, 36(3), 340-352.
(9) Moceri-Brooks, J., Garand, L., Sekula, L. K., Zoucha, R., & Joiner, T. (2024b). The Purple Heart and suicide risk in Post-9/11 US Army Combat Veterans with a traumatic brain injury: A mixed methods study. Military Psychology, 36(4), 443-455.
(10) Horn, B. (2002). A self-evident truth: Special Operations Forces and intelligence in asymmetric warfare. The Army Doctrine and Training Bulletin, 5(4), 20-20.
(11) Horn, B. (2003). Complexity squared: Operating in the future battlespace. Canadian Military Journal, 4(3), 8.
(12) Horn, B. (2004a). Bastard sons: An examination of Canada’s airborne forces, 1942-1995. National Library of Canada/Bibliothèque nationale du Canada, Ottawa.
(13) Horn, B. (2004b). Special men, special missions: The utility of special operations forces–a summation. Force of Choice: Perspectives on Special Operations. McGill-Queen’s Press-MQUP.(is duplicate number 12 above but didn’t want to mess up the numbering!)
(14) Horn, B., & Colonel, C. A. (2004). When cultures collide: The conventional military/SOF chasm. Canadian Military Journal, 5(3), 3-16.
(15) Last, D., & Horn, B. (Eds.). (2005). Choice of force: Special operations for Canada (Vol. 2). McGill-Queen’s Press-MQUP.
(16) Horn, B. (2005). The Dark Side to Elites: Elitism as a catalyst for disobedience. Canadian Army Journal, 8(4), 65-79.
(17) Horn, B. (Ed.). (2006). The Canadian way of war: serving the national interest. Dundurn.
(18) Horn, B., & Balasevicius, T. (Eds.). (2007). Casting light on the shadows: Canadian perspectives on special operations forces. Dundurn.
(19) Horn, B. (2007). “Love ‘em or Hate ‘em”: Learning to Live with Elites. Canadian Military Journal, 8(4), 2007-2008.
(20) Horn, B. (2010). No Lack of Courage: Operation Medusa, Afghanistan. Dundurn.
(21) Day, D. M., & Horn, B. (2010). Canadian special operations command: the maturation of a national capability. Government of Canada: Ottawa, Ontario.
(22) Horn, B. (2011). From Cold War to New Millennium: The History of The Royal Canadian Regiment, 1953–2008. Dundurn.
(23) Horn, B., & Spencer, E. (Eds.). (2012). No Easy Task: Fighting in Afghanistan. Dundurn.
(24) Horn, B. (2014). A reflection on leadership: A comparative analysis of military and civilian approaches. Journal of Military and Strategic Studies, 15(3).
(25) Horn, B. (2014). The strategic utility of special operations forces. Canadian Military Journal, 14(4), 66-70.
(26) Horn, B., & Bentley, B. (2015). Forced to change: Crisis and reform in the Canadian Armed Forces.
(27) Horn, B. (2016). No Ordinary Men: Special Operations Forces Missions in Afghanistan.
(28) Horn, B. (2016). Shadow Warriors/Les Guerriers de l’Ombre: The Canadian Special Operations Forces Command/Le Commandement des Forces d’Opérations Spéciales du Canada.
(29) Horn, B. (2016). A Most Ungentlemanly Way of War: The SOE and the Canadian Connection.
(30) Horn, B. (2017). The evolution of SOF and the rise of SOF Power 1. In Special Operations Forces in the 21st Century (pp. 15-27). Routledge.
(31) Horn, B. (2018). Nous trouverons un moyen: histoire des forces d’opérations spéciales du Canada.. Dundurn.
(32) Larkin, F.J. (2013). Vice Director Frank Larkin delivers remarks on “The Future of Joint Improvised Explosive Device Defeat Organization (JIEDDO). The Institute for Defense and Government Advancement (IDGA) Conference.Washington, DC.
(33) Larkin, F.J. in Starks, T. (2017). Who’s next to lead the FBI, and the cybersecurity ramifications. https://www.politico.com/tipsheets/morning-cybersecurity/2017/05/whos-next-to-lead-the-fbi-and-the-cybersecurity-ramifications-220257
(34) Larkin, F.J., in Lesniewski, N. (2018, Feb 26). Senate Sergeant-at-Arms Frank Larkin to Retire. Roll Call. https://rollcall.com/2018/02/26/senate-sergeant-at-arms-frank-larkin-to-retire/
(35) Larkin, F.J., in Derrick Van Orden Introduces Warrior Call Day Resolution, Co-Chairs Military Mental Health Task Force (2023a). Federal Information & News Dispatch, LLC.
(36) Larkin, F.J., in Van Orden’s Warrior Call Resolution Passes House (2023b). Federal Information & News Dispatch, LLC.
(37) Larkin, F.J., in Warren leads senate hearing to urge department of defense to better protect service members from weapon blasts (2024). Washington, DC: Federal Information & News Dispatch, LLC.
(38) Larkin, F.J., Rocklein, K.J., Moceri-Brooks, J. (2024, Mar 9). Expert testimony on traumatic brain injury and blast exposure care strategy: Hearing before the United States Senate Armed Services Committee, 118th Congress. https://t.ly/GLzuK
(39) Rocklein, K.J., Larkin, F.J., Moceri-Brooks, J. Military Suicide and Traumatic Brain Injury: Analysis & Recommendations for 2025 National Defense Authorization Act (NDAA). Submitted by request to the United States Senate Armed Services Committee, 31 Jan 2024.
(40) Rocklein, K.J., Larkin, F.J., Moceri-Brooks, J. Critical Review of the Warfighter Brain Health Initiative (WBHI) and Longitudinal Medical Study on Blast Pressure Exposure of Members of the Armed Forces. Submitted by request to the United States Senate Armed Services Committee, 1 Mar 2024.
(41) Rocklein, K.J., Larkin, F.J., Moceri-Brooks, J., with Warren, E., and Ernst, J. Blast Overpressure Safety Act, S. 4109 and H.R. 8025, 118th Congress. (2024, April 14). https://www.govtrack.us/congress/bills/118/hr8025/text
(42) Rocklein, K., Cook, D.J., Moceri-Brooks, J., Ditzel, R.D. (2025, May). Early detection of neurodegeneration and suicidality in Special Operations Forces: Future-phase epigenetic applications and initial validation of the FLARES-1 scale. Podium presentation, Special Operations Medical Association Scientific Assembly, Raleigh, USA.
(43) Rocklein, K. & Moceri-Brooks, J. (2025, May). Critical analysis of the Warfighter Brain Health Initiative and Longitudinal Blast Overpressure Study: Implications for future research and treatment of blast-exposed Special Operations personnel. Podium presentation, Special Operations Medical Association Scientific Assembly, Raleigh, USA.
(44) Rocklein, K. (2025, April). Combat-Related Overpressure Wave Neurotrauma and Sequelae: Strategic Implementation of the Blast Overpressure Ottawa Model for Rapid Harmonization of Multinational Efforts. Invited Speaker, NATO Science and Technology Symposium, Toronto, Canada.
(45) Ho, T., Rocklein Kemplin, K., Brandon, J. (2019). Testicular cancer in an American Special Forces soldier: A case report. The Journal of Special Operations Medicine, 19(1), 38-42.
(46) Rocklein Kemplin, K., Paun, O., Sons, N., & Brandon, J. (2018). The Myth of Hyper Resilience: Evolutionary Concept Analysis of Resilience in Special Operations Forces. The Journal of Special Operations Medicine, 18(1),54-60.
(47) Rocklein Kemplin, K., & Bowling, F.Y. (2017). Liberating the Oppressed: Research Knowledge Differentials and Ethical Investigation in Special Operations Clinical Science. The Journal of Special Operations Medicine, 17(1),7-11.
(48) Rocklein Kemplin, K., & Bowling, F.Y. (2017). Foreign Language Short Course: Special Operations Clinical Research Fundamentals. The Journal of Special Operations Medicine, 17(2),12-15.
(49) Rocklein, K. (2014). A Call for Innovation: Reflective Practices and Clinical Curricula of US Army Special Operations Forces Medics. The Journal of Special Operations Medicine, 14(4), 70-80.
(50) Rocklein Froede, K. (2011). Unconventional Medicine: The Genesis of Tactical Emergency Medicine and Indications for Special Operations Knowledge Exchange. Special Weapons and Tactics, 2011, 6-9.
(51) Rocklein Froede, K. (2011). Soldiers Can Take It: A Conceptual Analysis of Trauma. The Journal of Special Operations Medicine, 11(1), 18-22.
(52) Rocklein Froede, K. (2011). No shit, there I was: The Case for Narrative-Based Clinical Knowledge. The Journal of Special Operations Medicine, 11(4), 21-26.
(53 Meleis, A. I., Sawyer, L. M., Im, E. O., Messias, D. K. H., & Schumacher, K. (2000). Experiencing transitions: an emerging middle-range theory. Advances in Nursing Science, 23(1), 12-28.
(54) Meleis, A. I. (2010). Transitions theory: Middle range and situation specific theories in nursing research and practice. Springer Publishing.
(55) Im, E. O. (2014). Situation-specific theories from the middle-range transitions theory. Advances in Nursing Science, 37(1), 19-31.
(56) Peterson, S., & Bredow, T. S. (2019). Middle range theories: Application to nursing research and practice. Lippincott Williams & Wilkins.
(57) Im, E. O., & Meleis, A. I. (2021). Situation-specific theories: philosophical roots, properties, and approach. In Situation specific theories: development, utilization, and evaluation in nursing (pp. 13-27). Springer International Publishing.
(58) Rodgers, B. L. (1989). Concepts, analysis and the development of nursing knowledge: the evolutionary cycle. Journal of Advanced Nursing, 14(4), 330-335.