




The Time for Military Senior Leadership to Adopt a Trauma Leadership Model is Now

The Time for Military Senior Leadership to Adopt a Trauma Leadership Model is Now
By Don Bolduc
Everything I am seeing regarding Trauma Informed Leadership is in relationship to healthcare in the civilian sector… not any broader arena and I believe this is an oversight. I see applicability for a Trauma Leadership Model in many areas of our society and in all our institutions. This article will focus on the military. I want to thank all the hardworking and dedicated trauma healthcare professionals for their dedication and life saving efforts. Nothing contained in this article is intended to diminish them.
The current military leadership training serves the military well, but only brings the leadership so far and falls short in dealing with the leadership challenges involving trauma with their service members or the way trauma adversely affects leadership. In fact, the current doctrine might work fine in peacetime, or if there was/is a never-ending supply of “fresh legs” but that is not the case. This all-voluntary force has been sent back to War repeatedly and those who did not go to War were serving in an operational climate supporting warfighters, which is stressful and taxing in and of itself.
In light of 20 years of War, fought across multiple theaters of operation by the first all-voluntary force in the history of our country, a leadership paradigm shift that incorporates trauma informed leadership is not just warranted, it is essential to the health, resiliency and sustainability of our military service members and their families.
I believe that with CAREFUL presentation the concept of Trauma Informed Leadership can/will appeal to a broader base because it will speak to everyone and have a desired outcome of resiliency and readiness. This is a benefit/strength/skill set generated by my 33 plus years of military service from private to general and 81 months in combat. I am not a health care professional or trained counselor. The observations in this article are mine and should not be attributed to anyone else.
Although common to other areas of our society, there is no other profession that has dealt with trauma more so than the military. Trauma in the military is physical, mental, and spiritual and occurs from combat, moral injury, military sexual trauma, and toxic leadership, both on, and off the battlefield. The history of civilization is replete with examples of battlefield trauma.
In the field of trauma treatment, the military has always looked at mental injury as a weakness. Even what the military has called it throughout history is indicative of the institutional view of mental injury. In World War I they were shell shock. In World War II and Korea, it was called psychiatric collapse. In Vietnam and beyond, it is referred to as post-traumatic stress disorder. The “disorder” part is what service members do not like. What has not changed, is the stigma and the negative consequences of that stigma in the military and in our society across all combat veteran eras.
Wartime trauma effects every aspect of a given society. Whether it is the trauma experienced by the individual soldier, the civilians where war visits, or family members waiting at home, the resulting trauma of wartime operations is forever present and becomes part of the fabric of larger society.
History shows that the military has always been slow to recognize the negative effects of trauma on resiliency and readiness. The iconic scene in the movie “Patton” slapping a soldier has dictated the military approach to dealing with mental injury. Why? The idea of psychological weakness is antithetical to military culture with its ethos of strength and invulnerability. The mental disorders are not tangible and have no visible physical signs. The military approach to mental injury is largely process focused, checklist driven, and survey driven. Military service members and veterans have become very experienced at fooling them. I believe that it is impossible for our service members directly exposed to war not to be scarred and negatively affected their experiences.
The fear in the military is that trauma treatment may interfere with the warrior spirit and have negative effects on the aggressiveness required to close with and destroy the enemy. There is no proof that treatment for mental injury negatively impacts the will to fight. My personal and professional experience is the exact opposite. Treatment supported by senior leaders results in a more resilient, ready, and productive service member.
Studies done by RAND show that the “will to fight” is a hugely important human factor often overlooked by senior military leaders. “Recent failure to translate military gains into strategic success reflects, to some extent, the Joint Force’s tendency to focus primarily on affecting the material capabilities — including hardware and personnel — of adversaries and friends, rather than their will to develop and employ capabilities. A failure to grasp the human aspects can, and often will, result in a prolonged struggle and an inability to achieve strategic goals.”
Direct involvement by leaders is required to ensure trust, optimal resiliency, and readiness of the most critical combat multiplier, our people. History has shown that the most effective factor on the battlefield is the soldier and the leader. The calculus most often in winning is people. If our service members do not believe their leaders will support them, they will not go for help. The process must be leader driven.
There has been a recent emphasis on Trauma Informed Treatment and Trauma Informed Leadership in the medical profession. I believe these same “Trauma Informed Leadership” concepts utilized in the health care profession offer a viable alternative strategy to military leaders as well. Mental injuries in combat and the trauma associated with it is a natural response by the brain to keep you alive more than one day in combat. Your brain re-orders itself to the dangerous environment of combat. This is a cumulative affect and when you go back repeatedly as our service members have over the last 20 years the trauma becomes a natural way of acting. This is functional in combat, but when you come home it is problematic.
My trauma informed leadership experience caused me to approach physical, mental, and spiritual trauma in my division level command much differently than I had in the past.
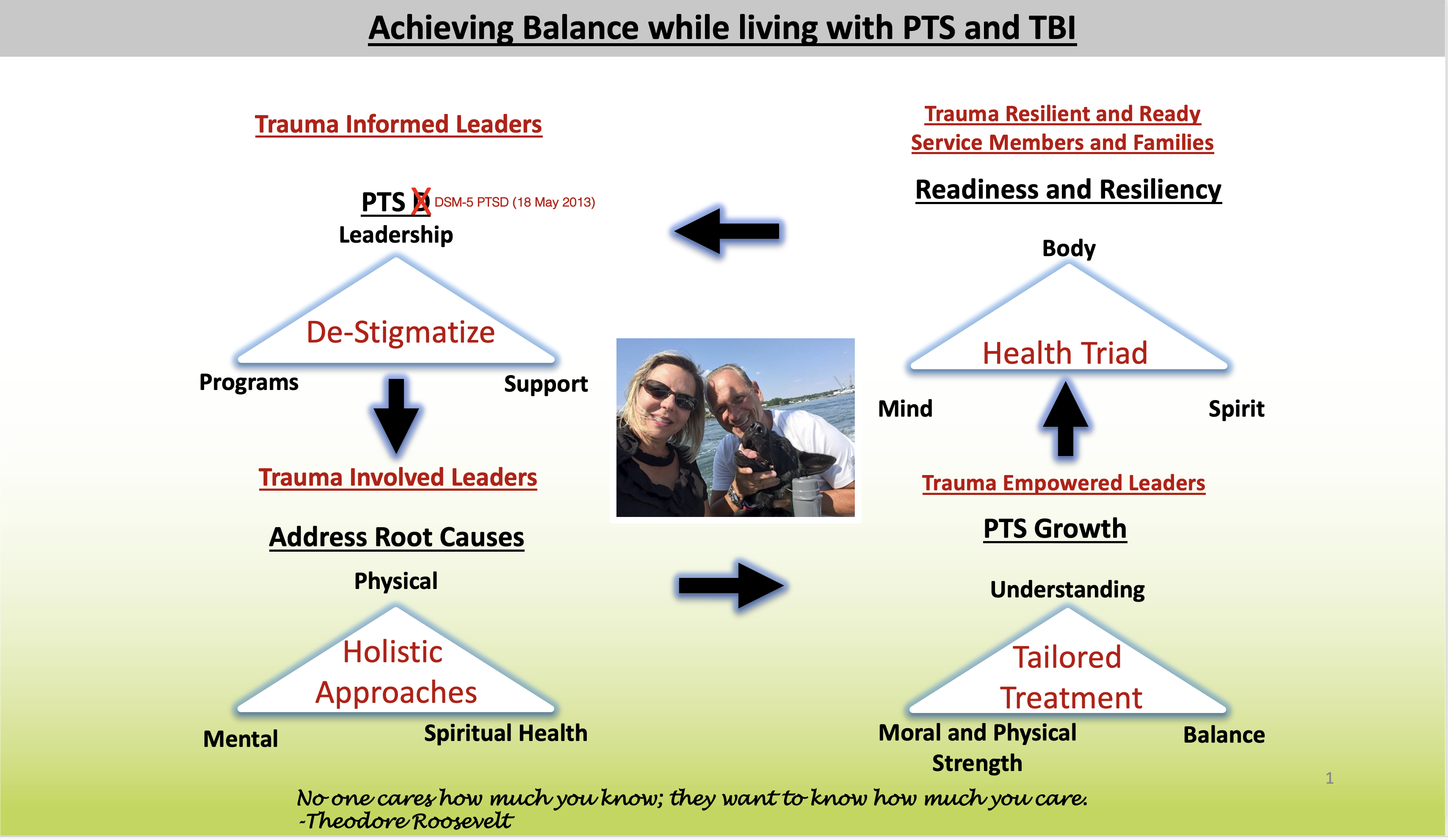
The goal of the Trauma Informed approach and applying it to the military will improve resiliency and readiness, improve interpersonal relationships, lead to better outcomes, and offer a positive perspective when facing difficult decisions. I have taken the trauma informed approach and expanded it to the following:
- Trauma informed leaders
- Trauma involved leaders
- Trauma empowered leaders
- Trauma resilient and ready service members, veterans, and families
The program we implemented in Special Operations Command-Africa was simple. It was command driven and underwritten by the commanding general and the senior enlisted adviser Master Chief (Navy SEAL) Richard Puglisi. We promised all our service members that they would stay in their jobs, they would not lose their clearances, and we would provide them top cover. We were true to our word despite pressure from the chain of command above me and the fact that I was taking a different approach than Department of Defense policy on handling personnel that self-identified with post traumatic stress and TBI and wanted treatment. Nurse Sarah McNary assisted the command in establishing a three-day assessment, evaluation, and tailored treatment program for every service member. The program put in place had minimal impact on the mission. It did have maximum benefits for people and families.
After implementing a program in conjunction with Landstuhl Regional Medical Center with Nurse Sarah McNary we achieved a significant level of success in treatment within Special Operations Command-Africa. What this trauma informed leadership approach did for me was significantly improved my personal and professional life. It allowed me to also provide the same for my service members and their families struggling from physical, mental, and spiritual trauma. This was huge.
Over a 26-month timeframe our alcohol and drug issues decreased, inappropriate behavior in the workplace decreased, suicidal ideations decreased, family issues decreased, and trust in the chain of command increased significantly. Most importantly, it informed us how to deal with personnel issues in the command much differently and more effectively.
There have been millions of taxpayer dollars spent on studies and consistently the data demonstrates that trauma related injury is not treated effectively. Senior military leadership are dealing with issues directly related to the consequences of trauma and following a model that is not having optimal results.
I believe a different leadership approach is required to handle the problem effectively. The current approach has failed to effectively address trauma related drug and alcohol abuse to self-medicate, behavioral issues, sexual assault and harassment in the workplace, family violence issues, divorce, and worst of all suicide. All these problems exist among our veterans in large part because they never received the appropriate treatment on active duty. Additional negative outcomes among our veterans are homelessness, unemployment, and incarceration.
The current USSOCOM commander has commissioned a study on the effects of repetitive, low level blast exposure on Special Operations Forces service members (ReBLAST). This is a move in the right direction, and it is good he is asking these questions. The key will be what is done with the results when the study is evaluated.
There are many health care professionals and leaders working hard to deal with trauma. They need additional assistance to use their skills inside a system that will achieve trust, optimal resiliency, and readiness. My experience and research suggest that a Trauma Senior Leadership Model is what is missing in the military to deal effectively with the traumatic effects of combat and other service-related trauma. Likewise, this must change in the veteran administration and is applicable to many other areas in our society.
We need our senior leaders to realize the powerful impact that a change in their mindset would have on the resiliency, readiness, morale, and quality of life of their service members while serving and as veterans. I have always said that if a leader cannot take care of himself/herself they have no business taking care of anybody else.
It’s my conclusion through experience, knowledge, and understanding that when service members and their families see their leadership personally invested, they will get the help they need.