Suicidal Ideation Assessment Among Intelligence Professionals
James Covey
My spirit is broken, my days are cut short, the grave awaits me.
-- Job 17:1
The idea of death is disturbing. More disturbing still, is the idea of suicide. Consequently, suicidal ideation (SI) is probably one of the most difficult challenges Army leaders grapple with. In this generation of the Army, SI trends across every echelon of the force have generated countless studies and programs. However, despite the ubiquitous nature of this dynamic, its unique impact on intelligence professionals should be of particular interest to Army leaders. In response to an uptick in reported SI in the 470th MI BDE, the BDE CDR directed the BDE Chaplain and Military and Family Life Consultant (MFLC) to develop a survey and assessment tool for her formation. That survey was piloted in the BDE’s HHC on 21 DEC 2017 and is currently being conducted in subordinate battalions.
Methodology
SI is simply defined as thinking about, considering, or planning suicide[i]. The broadness of that definition is part and parcel of its complexity for there is a profound difference between simply thinking about suicide and pursuing a plan for its completion. This reality was noted in a teleconference with Army G1 Suicide Prevention Program personnel subsequent to the survey where it was suggested that there should be a distinction between treating and reacting to SI with intent as opposed to SI without intent. That distinction can be too easily ignored as gatekeepers respond to SI (usually out of fear) and offer a one size fits all approach. This question was at the heart of the BDE CDR and CSM’s reflections as they sought insight not only on the journey of treatment and recovery for Soldiers, but also on the impact to intelligence operations when Soldier’s work site access is affected by their treatment. Fundamentally, the CMD Team was not concerned about institutional processes and talking points, but rather in the actual perceptions held by their Soldiers on this topic.
Online surveys are commonly accessed for these types of research questions. However, Soldiers (to say nothing of the general population) struggle with survey fatigue since the seemingly simplest transactions (an example of which in the Army would be getting one’s teeth cleaned) cannot be executed without a requirement to answer a digital survey. Moreover, Soldier’s cannot be required to navigate to a non-DoD website. These constraints led the Chaplain and MFLC to develop a hard copy survey that the formation could be invited to complete in real time. The survey was executed in coordination with quarterly ACE Training and Soldiers were directed to sources of care and response should the mere mention of the topic stir up anxiety. This forum also provided a more random survey population than the possibility that only Soldiers with a particular interest in the topic would chose to complete an online survey. Anonymity was guaranteed and the actual assessment took about 10 minutes. Soldiers could opt out of filling out the survey if they chose. It appeared everyone in the room completed the survey resulting in a total of 39 participants. After the survey was completed, a staff member had volunteered to give her personal testimony of her father’s suicide when she was ten years old. Taken together, the training and the survey offered a powerful experience of insight into the ramifications of a completed suicide on an individual and a family.
The quantitative section of the survey was easily calculated into percentages and pie charts. Answers to the survey’s qualitative section (probably the most useful responses of the assessment tool) were grouped into like themes. The Chaplain and MFLC both agreed on the groupings to evaluate emerging themes.
Quantitative Results
In terms of basic demographic questions that interested the CMD Team, 72% of survey participants were male and 54% noted that their home state was in the South. 15% were between the ages of 20 and 29 and 69% noted the socio-economic status of their family of origin as middle class. 54% (over half) of the respondents admitted having experienced SI. That experience occurred at an average age of 24. While that number might seem large, consideration of the broad definition of SI offers insight into the number of affirmative responses. This also supports the contention that SI is not an uncommon phenomenon. The burden is to assess the intent of SI.
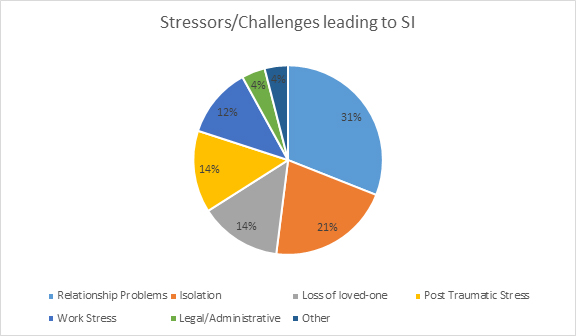
In broader Army studies of suicide, suicide attempts, and SI, the principal issues reported that were tied to this challenge were relationship, work, physical health problems, and victimization by abuse[ii]. The 470th MI BDE survey added isolation as a stress factor. The CMD Team theorized that the personality preferences and profile of intelligence analysts might exacerbate SI. Isolation was posited as a life stressor not as a judgment on a personality preference for introversion, but rather a kind of long term emotional compartmentalization and isolation that inhibits social intercourse and potential healthy interaction. Compartmentalization is a word that is certainly not foreign to intelligence professionals. It is in fact a requirement for operational security. However, integration both internally in one’s soul as well as externally in one’s most intimate relationships is considered a mark of health and wellness. As hypothesized, isolation was listed by Soldiers as the number 2 factor in their experience with SI.
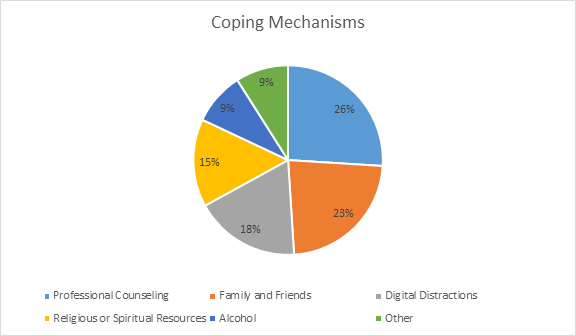
Coping mechanisms and sources of help were also assessed. Professional counseling as well as family and friends were expected to be a common source of help. However, the 470th team had again hypothesized that in the millennial generation, distraction through the internet, online gaming, and social media might be seen as source of coping. It was no surprise to then find that 18% of the respondents noted that this type of distraction was their default response to SI.
The distracting nature of life lived on digital platforms is a topic that certainly bears more study in the general population and in its particular impact on intelligence professionals. In 2010, Nicholas Carr published his bestselling book, The Shallows: What the Internet is Doing to our Brain[iii]. The book would eventually become a finalist for the Pulitzer Prize and Carr has subsequently authored several other books on the topic. The theory is that while living our lives on digital platforms, our brains develop the skills to toggle quickly from one task to another…what some call multitasking. There is utility in that skill. However, focusing on this task ignores and in a sense atrophies the other parts of our brain that are needed to pursue higher functions. Those brain functions are associated with feelings of satisfaction in one’s life and finding meaning and purpose. The net result of this digital conundrum is that we are developing and enhancing shallow lives. This is directly related to the internal tools and coping mechanisms Soldiers have or need to develop to deal with SI. A shallow toolbox of coping schools will inevitably leave one wanting in the crisis of SI. Added to the shallow nature of relationships that are cultivated through the digital platforms of social media, distraction as a coping resource should properly be seen as a risk rather than a help.
One of the good news stories of the survey was that among those who had received professional treatment for SI, more than 8 of 10 reported that it helped. That represents a tremendous validation to the investment the Army has made not only to behavioral health, but also to suicide prevention programs like ACE and ASIST. That investment will need to continue because 67% of survey respondents noted that they had had a close relationship with an Army coworker or battle buddy who had experienced SI. Tragically but tellingly, 36% had had a close relationship with someone in the Army who had completed a suicide.
Qualitative Results
The qualitative section of this survey may have yielded its richest results. Soldiers were asked to answer each question with narrative responses limited to 3 sentences or less. In reporting out the results of the survey, similar questions were grouped together according to theme. The qualitative questions and results are listed below:
- What do you think would happen to your clearance if you self-reported suicidal ideation in an effort to receive care and treatment?
- What do you think would happen to your work-site access if you self-reported suicidal ideation in an effort to receive care and treatment?
Four basic categories of response were offered for these questions. The largest group of responses (35%) clearly articulated a perception that there would be no change in either a Soldier’s security clearance status or work site access if a Soldier self-reported for SI. 26% stated that their clearance would be revoked. 23% thought there would be a potential or temporary loss of their clearance and work site access completely dependent on their circumstances or the course of their treatment for Si. 15% noted that their only concern was about the perceptions of leaders and peers (and their self-perception) rather than any concern for loss of clearance or access.
Beyond current security clearance and work site access perceptions, survey participants were next asked to think about the broader effect of SI on an Army Career.
- What do you think would happen to your Army Career if you self-reported suicidal ideation in an effort to receive care and treatment?
Once again, four broad categories of response were evident. 38% of respondents believed there would be absolutely no impact on a full, Army career if a soldier self-reported for SI. Diametrically opposed to this, another 38% stated that there would be negative impact on their career. 13% perceived that their career would be put on hold and 10% simply did not know what that consequence would be.
The next question was offered to survey a negative perception that some Army leaders have held with regard to the issue of malingering.
- Would you ever consider using suicidal ideation as an excuse to get out of work or any other Army requirement…or to avoid the consequences of adverse actions?
Responses to this question drew the strongest answer with 92% responding that they would never use SI as a tool to get out of work or detour out of the consequences of adverse actions. Only 5% admitted that they would use SI as an excuse, and 3% did not know if they would ever malinger.
The last section of the qualitative portion of the survey gave Soldiers an opportunity to share freely any perceptions or comments associated with the issue of SI. Themes of Soldier responses included reflections regarding the inevitability of SI as a consequence (in general) of the human condition…negative stigma’s that would follow Soldiers should they seek care (a common refrain)…as well as the seriousness with which this issue should be handled.
Several other themes flowed consistently through the qualitative portion of the survey. Responses seemed to indicate that Soldiers took this survey seriously and responded genuinely such that there appeared to be a high degree of validity and reliability to the survey (more iterations of the survey will be able to validate this). Perceptions regarding consequences of self-reporting SI tended toward either extreme for each question despite the reality that the most realistic consequences tend to be more subjective and circumstantial. Another common theme focused on fear of perception (by leaders, peers, and themselves) over actual institutional consequences. This of course is the stigmatization challenge that is so difficult to affect. Reflection and discussion on survey results between the CMD Team, Chaplain, and MFLC resulted in three broad insights.
Consequences are Not as Simple as They Seem
Fully 1/3rd of survey respondents believed that there would be absolutely no consequences of self-reporting for SI. While some of this perception is inevitable due to “barrack psychologists”, other sources of misinformation, or simply ignorance, there is a strong possibility that all of the Army’s noble efforts at non-stigmatizing promotion of behavioral health may have resulted in the creation of a false narrative. Is it generally true that if Soldiers seek care and respond to treatment they will move forward in an Army career subsequent to SI or any other personal crisis? Yes. However, is it also true (especially in the universe of Military Intelligence) that there can be real changes in the potential status of a Soldier’s clearance and work site access if they self-report SI? Yes. It appears that this is a reality that intelligence professionals are failing to communicate in an effort to react to the fear associated with SI. There are in reality large formations of Soldiers associated with many intelligence units who are in some kind of hold status precisely because of their current treatment. In effect, these Soldiers are in a kind of Warrior Transition Unit (WTU)…without any of the resources of an actual WTU. The second and third order effects of this are that unit leaders are not only tasked with their real-world missions, but also with all the complexities involved providing care and oversight to Soldiers in treatment. What’s worse, the Soldiers are literally “stuck” in a status where they cannot pursue their MOS, cannot be in fellowship and contact with friends, and thus are subject to an intensifying of many of the risk factors than can actually exacerbate SI. While admitting this reality is sobering and certainly comes with risk, honesty and candor might go a long way to more serious and measured responses to SI.
Guard Against Ignorance and Arrogance
Like most things in life, ignorance leads to arrogance. With regard to SI, survey participants tended toward perspectives in the extreme. 38% of respondents believed there would be absolutely no impact on a full, Army career if a soldier self-reported for SI. That exact percentage (38%) conversely believed the exact opposite would occur. It turns out that the truth is probably somewhere in the middle on this issue and most Soldiers are uninformed and under-educated…thus the tendency toward extreme perceptions. The truth is that the career of a Soldier affected by SI can follow many trajectories. The Army’s tendency toward appropriately highlighting success stories may incur the risk of silver lining a complex issue. The truth may be more subjective and is always more dependent on circumstances. Moreover, explaining this reality should not be rushed.
Rather than rehashing platitudes and generalization regarding outcomes and hoped for end-states, Army leaders should emphasize those responses that can actually mitigate risk such as accessibility to care and treatment. And they should not be afraid to soberly and compassionately assess each case of SI uniquely. Army G1 Suicide Prevention Program professionals suggest that SI will inevitably be a tool on the coping shelf that some Soldiers will turn to in a crisis or state of depression or loss. If that Soldier has other tools on that shelf beyond SI, there may be less risk. If that is the only tool on the shelf, there is greater risk. However, if that is the only tool on the shelf and there is intent, the risk may be imminent. A challenge as great as SI cannot be dealt with merely through public health campaigns for this is an issue of the human soul that must be attended to, respected, and provided for one person at a time. As in all things, the greatest challenges and opportunities in leadership have to do with personal relationships as opposed to programs.
All of this is to say that leadership can be pivotal in personally guiding Soldiers through complicated systems for the best outcomes. The 470th CMD Team intends to integrate SI assessment tools and skills into a planned pre-command course for CO CDRs and 1SGs to dig deeper each Soldier’s situation at the outset of reported SI. This is planned to augment and BY NO MEANS replace the effective sources of treatment available through the Army’s robust behavioral health resources. It is also intended to more deeply integrate leadership into each Soldier’s unique needs. Currently, the BDE CDR and CSM lead monthly Care Councils (aided by special staff) to discuss each high risk Soldier’s situation with that Soldier’s CO CDR and 1SG. The BDE CDR expects Company leadership to be able to have mastery of each high risk Soldier’s specific life situation and care plan. The enduring lesson seems to be (as one Soldier cautioned in the survey) that the Army must take the issue of SI “seriously” but guard against “extreme” reactions (both systemic and personal reactions).
Trust Your Soldiers
Intelligence professionals in the Army should take great pride in their formations. For Soldiers to enter these demanding MOSs, they have already been assessed as holding a degree of intelligence, insight, and maturity that rival any of the organizations within our nation’s national security infrastructure. A key take-away from this survey is that Army leaders should have that same pride and trust in their Soldiers with regard to the challenge of SI. Fully 92% of survey respondents stated that they would never use this issue to game or manipulate the system. MI Soldiers are smart enough to understand what a complicated journey of consequences for each instance of SI can be. That is precisely why they have cynical and critical attitudes toward leaders who offer only overgeneralizations and platitudes on this issue. MI Soldiers have paid attention to the journey others have taken who have faced this challenge. They are gifted analysts and have gathered intelligence on how the Army processes this challenge. They know how to separate the wheat from the chaff. They understand complexity. They also understand that resolving this challenge can take time. They take suicidal ideation seriously and understand that there is a compassionate system with gifted providers in place to meet these needs. Leaders should consequently treat their Soldiers with respect and if a Soldier presents himself through self-reporting, leaders should operate on the assumption that the cry for help is real.
End Notes
[i] Retrieved on 14 FEB 2018 from https://www.cdc.gov/violenceprevention/suicide/definitions.html
[ii] SURVEILLANCE OF SUICIDE BEHAVIOR 2016 ANNUAL PUBLICATION. (U) (MCHB-PH-BSH) The U.S. Army Public Health Center, Division of Behavioral and Social Health Outcomes Practice, 2016 Surveillance of Suicidal Behavior Publication (SSBP)4 DEC 2017.
[iii] Carr Nicholas. The Shallows: What the Internet is Doing to our Brains. W.W. Norton & Company, 2010.