Maintaining Military Dominance in the Future Operating Environment: A Case for Emerging Human Enhancement Technologies that Contribute to Soldier Resilience
Joelle B. Thorpe, Kimberly D. Girling and Alain Auger
Overview
Developing soldiers who are resilient to physical and psychological injury and illness is an enduring military challenge that will continue to be encountered in the future operating environment (FOE). The intent of this paper is to present a sample of emerging human enhancement (HE) technologies that may contribute to soldier resilience by enabling soldiers to recover quickly from injury and illness, or to avoid injury and illness altogether. Enhancements for soldier resilience can come in many forms. Some examples are: advanced therapeutics or medical devices to more effectively treat illness or injury; emerging technologies to identify and alert soldiers to potential threats; and sophisticated machinery that modifies soldier capabilities to reduce the risk of injury. Considerable interest in HE technologies has been generated in part because they are so wide-ranging in their contributions to soldier resilience. As a result of this significant interest, science and technology advancements for HE are progressing rapidly and many new technological solutions that contribute to soldier resilience can be expected to emerge in the future. We conclude by presenting a case for the importance of identifying potential ethical issues with the use of HE technologies for soldier resilience as a way to facilitate their timely adoption by the military as the technologies become ready for use in the FOE.
The Future Operating Environment of 2050: Predictions and Assumptions
There has been a relatively recent yet dramatic shift in the distribution of the world’s population: until 2007, the majority of people lived in rural versus urban centres; since then, the proportion of the world’s population residing in urban areas has continued to increase, reaching 54% in 2014 and projected to reach 66% by 2050 [1]. As a result of this persistent demographic shift, the FOE in which militaries will need to engage is likely to be characterized by dense, urban areas [2]. The urbanization of the FOE presents challenges to the U.S. military [3]. For example, fighting in close quarters means that soldiers may have to leave their vehicles to achieve their objective, putting them at greater risk of attack; congestion may block the movement of army vehicles, increasing their likelihood of being successfully targeted; and casualty evacuations may be delayed, putting soldier and civilian lives at risk [4]. Moreover, the unruly, noisy nature of these dense urban areas may intensify physical and cognitive fatigue in soldiers [5], which could lead to confusion and poor decision-making resulting in injury. Because of these and other challenging factors, the FOE of 2050 is predicted to be complex and chaotic [6], and this is a concern for the U.S. military [7].
In order to maintain dominance in this FOE, the U.S. military will continue to invest in research and development (R&D) to retain technological superiority over adversaries, as outlined in the Third Offset Strategy [8,9]. Specifically, the Department of Defense sees advancements in artificial intelligence (AI) and autonomous systems as the next breakthroughs for maintaining technological superiority. AI that enables soldiers to gather and analyze massive amounts of information rapidly to identify targets, and autonomous systems that enable soldiers to achieve their objectives while remaining further from dangerous zones will both certainly be advantageous in the dense, chaotic, urban operating environment of 2050. Regardless of the technologies the U.S. military has at its disposal, however, adversaries will continue to find ways to counter them. A technologically superior military can still be challenged by homemade and relatively simple devices such as improvised explosives. Moreover, advanced technologies are becoming cheaper and more accessible, making it easier for adversaries to obtain and use them against the U.S, and more difficult for the U.S. to maintain its technological edge. These facts have led some to conclude that technological superiority may not be sufficient to maintain military dominance in the FOE [10]. Instead, “technology…is only a tool and symptom of the problems the U.S. will be called upon to face – at the core of current and future conflict are people” [10]. In other words, war will remain a fundamentally human enterprise in the FOE, and this should not be ignored by focusing solely on technology as a way to maintain dominance.
If we accept the reasonable prediction that warfare will remain human-centred in the FOE, it follows that in times of conflict soldiers will always be needed on the ground (and at sea, in the air, and in cyberspace), risking their lives. Furthermore, the characteristics of the urban FOE indicate that risks to future soldiers may even be greater than they are to soldiers today. Therefore, an enduring challenge encountered by the U.S. military will be to develop ways to improve resilience in soldiers. Resilient soldiers able to recover from injury and illness rapidly or able to avoid injury and illness altogether will be a key factor in maintaining military dominance in the FOE [11]. One way to improve soldier resilience is with the use of a number of emerging technologies. Although technological superiority in terms of advanced weaponry, intelligence-gathering, and communications may not necessarily create an invulnerable military for reasons described above, technological advancements that improve soldier resilience will always have utility for the U.S. military: physical and psychological risk to the soldier will always exist, and healthy, focused soldiers will always be necessary for military success. The importance of developing resilient soldiers is reflected in the large number of emerging technologies that contribute to soldier resilience; many of these solutions have been designed as human enhancement (HE) technologies.
Human Enhancement Technologies for Soldier Resilience
HE has been defined in several different ways in the literature. For example, some draw a distinction between therapy (restoring a human capacity to the species-typical level), and enhancement (going beyond the typical capacity of a human) [12,13], whereas others have pointed out that there are some issues with this distinction [14]. Although there is still some disagreement about its definition, there is a general consensus on the difficulty of coining a universal definition for HE. For the purposes of this paper, we have defined HE broadly as including any technology (drug or device) implanted, ingested, or worn closely to the body that temporarily or permanently modifies or contributes to human functioning. This definition includes therapeutic devices that mimic human biological capacities in a superior manner, in addition to those that augment human capacities beyond the normal range (regardless of whether it was used to restore functioning in an injured individual).
Although some HE technologies such as exoskeletons and robotic limbs may seem like something out of science fiction, our use of HE is not a new phenomenon. Vaccines, which can be considered enhancements because they enable the immune system to recognize and attack viruses that it otherwise might not, have been used for hundreds of years [15]. HE is also pervasive in society: wearable health monitors are popular and have been studied for their potential to improve health [16]; devices to enhance athletic performance and safety have been developed and commercialized [17,18]; and even healthcare professionals have shown an interest in using augmented reality glasses to assist with surgery [19,20]. There is undoubtedly widespread interest in HE, and this interest even extends beyond civilian society to the military.
There are several military and space research agencies in the U.S., including: the Army Research Laboratory; the Air Force Research Laboratory; the Office of Naval Research; the Defense Advanced Research Projects Agency (DARPA); and the National Aeronautics and Space Administration (NASA), which has a program specifically geared toward enhancing performance and mitigating risk to astronauts (the Human Health and Performance Research Program). One considerable area of investment at DARPA is HE R&D. Advancements in HE technologies are happening rapidly: by 2050 it has been predicted that there will be soldiers on the battlefield who have “exoskeletons, possess a variety of implants, and have seamless access to sensing and cognitive enhancements” [21]. There are many DARPA-funded HE projects currently underway and at varying stages of progress. These are detailed on the DARPA website and include programs to develop a pain vaccine (Electrical Prescriptions program), to develop neural interfaces that allow prosthetic limbs to be controlled with brain signals (Reliable Neural-Interface Technology program), and to develop implanted nanoplatforms that monitor physiological conditions of soldiers to detect disease or illness (In Vivo Nanoplatforms program). Some of the emerging HE technologies DARPA is interested in developing may serve to improve soldier resilience once they are introduced onto the battlefield.
Soldier resilience is defined by the U.S. Army as “the mental, physical, emotional and behavioral ability to face and cope with adversity, adapt to change, recover, learn and grow from setbacks” [22]. Developing resilient soldiers who are better able to avoid physical or psychological injury and illness, or who can recover faster from injury and illness has clear benefits for the U.S. military, for soldiers, and for soldiers’ families. For instance, resilient soldiers may be better able to: 1) recover faster and return to the battlefield after an injury or illness that might otherwise have resulted in their discharge; 2) maintain composure and focus during stressful situations on the battlefield, allowing them to achieve military objectives without incident; and 3) avoid psychological and/or physical injury and smoothly re-integrate into civilian life upon return from duty. The importance to the U.S. military of developing resilient soldiers is demonstrated by the inclusion of this issue on the list of Army Warfighting Challenges [11]. In the complex and chaotic FOE, having resilient soldiers will be integral to U.S. military dominance.
Resilience can be cultivated in soldiers in several non-mutually exclusive ways. The U.S. Army Ready and Resilient Campaign [23] includes the Comprehensive Soldier and Family Fitness Program, which teaches resilience and enhancement skills that enable soldiers to “cope with adversity, perform better in stressful situations and thrive in life” [22]. Another approach to developing resilient soldiers is the use of HE technologies that contribute to soldier resilience. HE technologies can contribute to soldier resilience in a number of different ways, including improved injury and illness prevention, detection, and/or treatment, improved soldier capabilities leading to reduced risk of injury, and improved threat detection allowing soldiers to avoid dangerous situations. The U.S. Army Operating Concept lists HE as a key technological area of focus for developing resilient soldiers who can thrive in the chaotic and dangerous FOE [2].
The U.S. military’s need to develop HE technologies that contribute to soldier resilience is evident in the amount of funding provided by the Department of Defense to research agencies like DARPA [24,25]. It is also evident in the vast number of existing and emerging HE technologies that may contribute to soldier resilience: see Table 1 for a sample of emerging and existing HE technologies currently in development and how they may contribute to soldier resilience in the FOE[i]. HE technologies offer numerous ways to contribute to soldier resilience.
HE technologies can be categorized based on whether they offer a physiological, computational, cognitive, automated, or robotic solution to soldier resilience [113]. These are not mutually exclusive, and many technologies fall into more than one category. Furthermore, a 9-point Technology Readiness Level (TRL) can be assigned to each of these technologies as a way to rate how close they are to being ready for use in an operational environment [114]. Technologies at the low end (1-3) are still in the proof-of-concept phase, technologies in the mid-range (4-6) are in the laboratory validation phase, and technologies at the high end (7-9) are being tested in operational environments. The majority of the HE technologies for soldier resilience in the small sample we surveyed are physiological, and they fall along the entire spectrum of TRL (Figure 1). However, it is clear from Figure 1 that most of the HE technologies we identified have low TRLs. That is, although some of these HE technologies may be ready for use on the battlefield in the near future, most of them are still in very early development phases, and therefore they will likely be more pertinent for soldier resilience in the FOE of 2050.
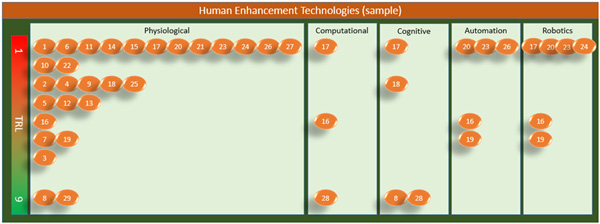
Figure 1: Sample of HE technologies grouped by HE category and TRL. Each number represents a technology listed in Table 1.
For as long as there are humans involved in conflict, resilient soldiers will continue to be a necessary qualification for success on the battlefield and in turn for military dominance. Emerging HE technologies being developed right now may contribute to soldier resilience in the future theater of operations. Because of the importance of maintaining soldier resilience and the promise of HE technologies in this realm, it is likely that new HE technologies that contribute to soldier resilience will continue to emerge in the future. However, whether we are envisioning military use of a HE technology for soldier resilience that currently exists or is merely hypothetical right now, there is at least one constant consideration that must be made: how to use HE technologies for soldier resilience in an ethical manner.
Military Ethics of Human Enhancement Technologies for Soldier Resilience
We ignore the ethical implications of HE technology use for soldier resilience at our own peril. Without proper a priori ethical considerations, the adoption of HE technologies could stall at the regulatory policy development stage, hindering the deployment of HE solutions for more resilient soldiers. Perhaps even more grave, if ethics is not considered prior to the adoption of HE technologies, unanticipated and potentially catastrophic unethical situations on the battlefield could ensue. Neither of these outcomes is desirable for military dominance in the FOE.
There is concern about the widening gap in our knowledge of the ethical, legal, and social issues associated with military use of HE technologies resulting from the disparity between the rapid progress of R&D and the slow pace of policy development [115-117]. This concern has led many to discuss the ethics of soldier enhancement in general [118-120], and others including ourselves to develop frameworks to facilitate the identification of potential ethical issues associated with the use of specific HE technologies by militaries [116,117,121]. Ideally, these frameworks will be used by both technology developers and policy-makers. Technology developers can use assessment frameworks early on to identify and mitigate ethical issues associated with a particular HE technology through design adjustments and later through the test and evaluation phase of the technology. Policy-makers can use assessment frameworks to identify ethical issues associated with the use of a particular HE technology and attempt to avoid these issues through the development of policies that safeguard ethical military use. In both cases, ethics assessments should serve to inform the development and ethical use of HE technologies for soldier resilience.
With the aid of an assessment framework developed by our research team [117], we identified potential ethical issues associated with the use of each HE technology for soldier resilience listed in Table 1 and Figure 1. It is reasonable to predict that less developed HE technologies with low TRLs might have more potential ethical issues compared to more developed technologies with high TRLs. Although our sample size is too small to draw firm conclusions, the most frequently identified ethical issues were raised by technologies with, on average, low TRLs. It is important to note, however, that ethical questions were raised by all HE technologies regardless of TRL. While ethical assessments of HE technologies at every stage of development are imperative, we recommend that particular attention be paid by policy-makers to those technologies with mid-to-high TRLs so that their adoption in the near future is not delayed. Furthermore, HE technologies with high TRLs will also be available to adversaries, raising the issue of mitigating emerging threats with proper countermeasures and their associated policies. Continual ethics assessments by developers of HE technologies with low TRLs will ensure that these newly emerging technologies for soldier resilience will be ready and compliant for ethical use in the FOE of 2050.
In general, the HE technologies for soldier resilience we identified in Table 1 raise many of the same potential ethical challenges. For instance, considerations of most HE technologies resulted in questions about how reliable and trustworthy they are for use in an operational environment – will they break down, putting soldiers at risk? They also raised questions about how their distribution and use might negatively affect unit cohesion – will unequal distribution of the technology between soldiers cause tension and lead to dysfunction? Further questions about how return to civilian life might be impacted were also identified – will a permanent technology give a veteran an unfair advantage or disadvantage at finding employment? Many soldier resilience HE technologies also raised health and safety questions – are there unknown side effects or long term effects that could lead to unanticipated health problems during deployment or after discharge? Moreover, is it ethical to force a soldier to use the technology in question, or should he/she be allowed to consent to its use? Can consent be fully free from coercion in the military? Important questions about who should be held responsible for a technology malfunction were also flagged – if a soldier on a drug to reduce fatigue who hasn’t slept in days kills an ally or civilian, is he/she responsible? Finally, many HE technologies for soldier resilience raise privacy and security concerns – who can view personal health data collected by the technology? Could the use of the technology make it easier for an adversary to locate and target a soldier, thereby putting him/her at risk? Although many of these questions do not have clear answers yet, they all require consideration to ensure that these HE technologies are used ethically in the FOE of 2050 or sooner.
Conclusion
A military is only as strong and effective as its warfighters; without soldiers who are able to withstand the pressures and dangers of conflict, it is challenging for any military to maintain its dominance. This is likely to be especially true in the dense, complex, and chaotic FOE of 2050. Although new technologies for warfare will continue to be created and used in the future by both allies and adversaries, highly trained soldiers will always be needed on the ground, in the air, at sea, and increasingly in cyberspace. Given the money and time investment put into developing and training soldiers, losing these highly skilled individuals to psychological or physical injury is undesirable. Soldiers who can resist injury or recover from it quickly and return to the battlefield have clear benefits not only for the military, but also, in the case of retiring soldiers readjusting well to civilian life, for society at large. The presence of these resilient soldiers in all 5 domains (ground, air, sea, space, and cyberspace) will certainly contribute to the U.S. military’s superiority in multi-domain battle in 2050 [122]. There is a substantial number of HE technologies in varying stages of development that may contribute to resilience in soldiers working in the FOE, a small selection of which we have highlighted in this paper. Although they offer many different possible ways to contribute to soldier resilience, several potential ethical issues associated with their use need addressing either through policies or design modifications before they can be adopted and used to improve resilience in soldiers. Proper and early consideration of the potential ethical problems arising with the use of HE technologies for soldier resilience will enable the U.S. military to adopt these technologies in a timely manner and use them effectively. Therefore, rather than impeding the adoption of emerging technologies, ethical assessments will better enable the U.S. military to take advantage of the benefits HE technologies may provide for soldier resilience in the FOE of 2050.
References
[1] United Nations Department of Economic and Social Affairs, Population Division. 2015. World Urbanization Prospects: The 2014 Revision.
[2] US Army Operating Concept – Win in a Complex World 2020-2040. TRADOC Pamphlet 525-3-1.
[3] Bailey M, Dixon R, Harris M, Hendrex D, Melin N, Russo R. Chief of Staff of the Army’s Strategic Studies Group. 2014. A Proposed Framework for Appreciating Megacities: A US Army Perspective. Small Wars Journal.
[4] Morrison DA, Wood CD. 2016. Megacities and Dense Urban Environments: Obstacle or Opportunity? Small Wars Journal.
[5] Hills A. Future War in Cities: Rethinking a Liberal Dilemma. New York, NY: Frank Cass, 2004.
[6] Amerson K, Meredith SB III. 2016. The Future Operating Environment 2050: Chaos, Complexity and Competition. Small Wars Journal.
[7] Harris M, Dixon R, Melin N, Hendrex D, Russo R, Bailey M. Chief of Staff of the Army, Strategic Studies Group. 2014. Megacities and the United States Army: Preparing for a Complex and Uncertain Future.
[8] Pellerin C. 2016. Deputy Secretary: Third Offset Strategy Bolsters America’s Military Deterrence. DoD News, Defense Media Activity. Accessed April 7, 2017: https://www.defense.gov/News/Article/Article/991434/deputy-secretary-third-offset-strategy-bolsters-americas-military-deterrence
[9] Work B. 2016. Deputy Secretary of Defense Speech: Remarks by Deputy Secretary Work on Third Offset Strategy. Delivered in Brussels, Belgium, April 28, 2016. Accessed April 7, 2017: https://www.defense.gov/News/Speeches/Speech-View/Article/753482/remarks-by-d%20eputy-secretary-work-on-third-offset-strategy
[10] Wood CD. 2016. The Human Domain and the Future of Army Warfare: Present as Prelude to 2050. Small Wars Journal.
[11] U.S. Army. 2017. Army Warfighting Challenges. Accessed April 7, 2017: http://www.arcic.army.mil/App_Documents/AWFC-Current.pdf
[12] Cabrera LY. Rethinking Human Enhancement: Social Enhancement and Emergent Technologies. New York, NY: Palgrave Macmillan, 2015.
[13] Allhoff F, Lin P, Moor J, Weckert J. 2009. Ethics of Human Enhancement: 25 Questions & Answers. Prepared for: US National Science Foundation.
[14] Bostrom N, Roache R. Ethical Issues in Human Enhancement. In: New Waves in Applied Ethics. Eds: Jesper Ryberg, Thomas Petersen, Clark Wolf. London, UK: Palgrave Macmillan, 2008; p. 120-152.
[15] Stern AM, Markel H. 2005. The History of Vaccines and Immunization: Familiar Patterns, New Challenges. Health Affairs 24: 611-621.
[16] Lewis ZH, Lyons EJ, Jarvis JM, Baillargeon J. 2015. Using an Electronic Activity Monitor System as an Intervention Modality: A Systematic Review. BMC Public Health 15: 585.
[17] Grahn DA, Cao VH, Nguyen CM, Liu MT, Heller HC. 2012. Work Volume and Strength Training Responses to Resistive Exercise Improve with Periodic Heat Extraction From the Palm. Journal of Strength and Conditioning Research 26: 2558-2569.
[18] Dingman S. 2014. Reebok’s Checklight Measures Hits to the Head. But is it Useful in Predicting Concussion? In: The Globe and Mail. Accessed April 13, 2017: http://www.theglobeandmail.com/life/health-and-fitness/health/is-reeboks-skull-impact-monitor-useful-in-predicting-concussion/article17498255/
[19] Chang JYC, Tsui LY, Yeung KSK, Yip SWY, Leung GKK. 2016. Surgical Vision: Google Glass and Surgery. Surgical Innovation 23: 422-426.
[20] Schreinemacher MH, Graafland M, Schijven MP. 2014. Google Glass in Surgery. Surgical Innovation 21: 651-652.
[21] Kott A, Alberts D, Zalman A, Shakarian P, Maymi F, Wang C, Qu G. 2015. Visualizing the Tactical Ground Battlefield in the Year 2050: Workshop Report. U.S. Army Research Laboratory: ARL-SR-0327.
[22] Warrior Care and Transition: U.S. Army Warrior Care. Accessed April 11, 2017: http://www.wct.army.mil/modules/soldier/s5-resilience.html
[23] U.S. Army Ready and Resilient Campaign. Accessed April 18, 2017: https://www.army.mil/readyandresilient/
[24] Jacobsen A. The Pentagon’s Brain: An Uncensored History of DARPA, America’s Top-secret Military Research Agency. United Kingdom: Hachette Book Group, 2015.
[25] Prabhakar A, Walker SH. 2015. Breakthrough Technologies for National Security. Defense Advanced Research Projects Agency Technical Report.
[26] Advanced Synthetic Probiotics Product Website. Accessed April 19, 2017: http://www.synlogictx.com/
[27] Sola-Oladokun B, Culligan EP, Sleator RD. 2017. Engineered Probiotics: Applications and Biological Containment. Annual Review of Food Science and Technology. 8: 353-370.
[28] Kang JH, Super M, Yung CW, et al. 2014. An extracorporeal blood-cleansing device for sepsis therapy. Nature Medicine. 20: 1211-1216.
[29] Hexoskin Product Website. Accessed April 19, 2017: https://www.hexoskin.com/
[30] Kumar A, Levin E, Cowing P, Toscano WB. Evaluation of the Accuracy of Astroskin as a Behavioral Health Self-Monitoring System for Spaceflight. Poster presented at the Annual Summer STEM Internship Symposium, Salinas California August 22, 2015. Accessed April 19, 2017: https://ntrs.nasa.gov/archive/nasa/casi.ntrs.nasa.gov/20150021842.pdf
[31] Montes J, Stone TM, Manning JW, et al. 2015. Using Hexoskin Wearable Technology to Obtain Body Metrics During Trail Hiking. International Journal of Exercise Science. 8: 425-430.
[32] Danino T, Prindle A, Kwong GA, et al. 2015. Programmable Probiotics for Detection of Cancer in Urine. Science Translational Medicine. 7: 289.
[33] Kotula JW, Kerns SJ, Shaket LA, et al. 2014. Programmable Bacteria Detect and Record an Environmental Signal in the Mammalian Gut. Proceedings of the National Academy of Sciences, USA. 111: 4838-4843.
[34] Shemer B, Palevsky N, Yagur-Kroll S, Belkin S. 2015. Genetically Engineered Microorganisms for the Detection of Explosives’ Residues. Frontiers in Microbiology. 6: 1175.
[35] Jia W, Valdes-Ramirez G, Bandodkar AM, Windmiller JR, Wang J. 2013. Epidermal Biofuel Cells: Energy Harvesting from Human Perspiration. Angewandte Chemie International Edition. 52: 7233-7236.
[36] Jeerapan I, Sempionatto JR, Pavinatto A, You J-M, Wang J. 2016. Stretchable Biofuel Cells as Wearable Textile-Based Self-Powered Sensors. Journal of Materials Chemistry A. 4: 18342-18353.
[37] Abreu MA, Edwards W, Spradley BD. 2016. The War Against Concussions. The Sport Journal. 19.
[38] Luna T. 2013. Mass. Companies Team Up to Prevent Head Injuries. The Boston Globe. Accessed April 19, 2017: http://www.bostonglobe.com/business/2013/07/14/reebok-introduce-concussion-sensor-for-sports/s7L509zIM5lBrHXb0ylDDM/story.html
[39] Liberman R. 2015. Reebok’s Checklight: A Standout in Wearable Devices. The Biotech Review. Accessed April 19, 2017: http://www.bostonbiotech.org/biotech-review/2015/6/8/reeboks-checklight-a-standout-in-wearable-devices
[40] Repantis D, Schlattmann P, Laisney O, Heuser I. 2010. Modfinil and Methylphenidate for Neuroenhancement in Healthy Individuals: A Systematic Review. Pharmacology Research. 62: 187-206.
[41] Marraccini ME, Weyandt LL, Rossi JS, Gudmundsdottir BG. 2016. Neurocognitive Enhancement or Impairment? A Systematic Meta-Analysis of Prescription Stimulant Effects on Processing Speed, Decision-Making, Planning, and Cognitive Perseveration. Experimental and Clinical Psychopharmacology. 24: 269-284.
[42] Sekins KM, Barnes SR, Fan L, et al. 2015. Deep Bleeder Acoustic Coagulation (DBAC) – Part I: Development and In Vitro Testing of a Research Prototype Cuff System. Journal of Therapeutic Ultrasound. 3: 16.
[43] Sekins KM, Barnes SR, Fan L, et al. 2015. Deep Bleeder Acoustic Coagulation (DBAC) – Part II: In Vivo Testing of a Research Prototype System. Journal of Therapeutic Ultrasound. 3: 17.
[44] Kim D-H, Lu N, Ma R, et al. 2011. Epidermal Electronics. Science. 333: 838-843.
[45] Webb RC, Bonifas AP, Behnaz A, et al. 2013. Ultrathin Conformal Devices for Precise and Continuous Thermal Characterization of Human Skin. Nature Materials. 12: 938-944.
[46] Norton JJ, Lee DS, Lee JW, et al. 2015. Soft, Curved Electrode Systems Capable of Integration on the Auricle as a Persistent Brain-Computer Interface. Proceedings of the National Academy of Sciences USA. 112: 3920-3925.
[47] Perry TS. 2015. Giving Your Body a “Check Engine” Light: Temporary Tattoos Can Replace Today’s Clunky Biomedical Sensors. IEEE Spectrum. 52: 34.
[48] Webb RC, Ma Y, Krishnan S, et al. 2015. Epidermal Devices for Noninvasive, Precise, and Continuous Mapping of Macrovascular and Microvascular Blood Flow. Science Advances. 1:9.
[49] Webb RC, Pielak RM, Bastien P, et al. 2015. Thermal Transport Characteristics of Human Skin Measured In Vivo Using Ultrathin Conformal Arrays of Thermal Sensors and Actuators. PLoS ONE. 10:2.
[50] Koh A, Kang D, Xue Y, et al. 2016. A Soft, Wearable Microfluidic Device for the Capture, Storage, and Colorimetric Sensing of Sweat. Science Translational Medicine. 8: 366.
[51] Liu Y, Norton JJS, Qazi R, et al. 2016. Epidermal Mechano-Acoustic Sensing Electronics for Cardiovascular Diagnostics and Human-Machine Interfaces. Science Advances. 2: 11.
[52] Pan D, Rogers S, Misra S, et al. 2016. Erythromer (EM), a Nanoscale Bio-Synthetic Artificial Red Cell: Proof of Concept and In Vivo Efficacy Results. Blood. 128: 1027.
[53] Miranda DL, Hsu WH, Gravelle DC, et al. 2016. Sensory Enhancing Insoles Improve Athletic Performance During a Hexagonal Agility Task. Journal of Biomechanics. 49: 1058-1063.
[54] Miranda DL, Hsu WH, Petersen K, et al. 2016. Sensory Enhancing Insoles Modify Gait During Inclined Treadmill Walking with Load. Medicine & Science in Sports & Exercise. 48: 860-868.
[55] Lipsitz LA, Lough M, Niemi J, et al. 2015. A Shoe Insole Delivering Subsensory Vibratory Noise Improves Balance and Gait in Healthy Elderly People. Archives of Physical Medicine and Rehabilitation. 96: 432-439.
[56] Gootenberg JS, Abudayyeh OO, Lee JW, et al. 2017. Nucleic Acid Detection with CRISPR-Cas13a/C2c2. Science. DOI: 10.1126/science.aam9321
[57] Bikard D, Euler CW, Jiang W, et al. 2014. Exploiting CRISPR-Cas Nucleases to Produce Sequence-Specific Antimicrobials. Nature Biotechnology. 32: 1146-1150.
[58] Maeder ML, Gersbach CA. 2016. Genome-Editing Technologies for Gene and Cell Therapy. Molecular Therapy. 24: 430-446.
[59] Cox DBT, Platt RJ, Zhang F. 2015. Therapeutic Genome Editing: Prospects and Challenges. Nature Medicine. 21: 121-131.
[60] Boland CS, Khan U, Ryan G, et al. 2016. Sensitive Electromechanical Sensors Using Viscoelastic Graphene-Polymer Nanocomposites. Science. 354: 1257-1260.
[61] Mannoor MS, Tao H, Clayton JD, et al. 2012. Graphene-Based Wireless Bacteria Detection on Tooth Enamel. Nature Communications. 3: 763.
[62] Asbeck AT, Schmidt K, Galiana I, Wagner D, Walsh CJ. Multi-Joint Soft Exosuit for Gait Assistance. IEEE International Conference on Robotics and Automation. Seattle, Washington, May 26-30, 2015.
[63] Panizzolo FA, Galiana I, Asbeck AT, et al. 2016. A Biologically-Inspired Multi-Joint Soft Exosuit That Can Reduce the Energy Cost of Loaded Walking. Journal of NeuroEngineering and Rehabilitation. 13:43.
[64] Quinlivan BT, Lee, S, Malcolm P, et al. 2017. Assistance Magnitude versus Metabolic Cost Reductions for a Tethered Multiarticular Soft Exosuit. Science Robotics. 2: 2.
[65] Stentrode Product Website. Accessed April 19, 2017: http://smartstent.com.au/about-us/
[66] Kwok R. 2013. Neuroprosthetics: Once More, With Feeling. Nature. 497: 176-178.
[67] Miranda RA, Casebeer WD, Hein AM, et al. 2015. DARPA-Funded Efforts in the Development of Novel Brain-Computer Interface Technologies. Journal of Neuroscience Methods. 244: 52-67.
[68] Bouton CE, Shaikhouni A, Annetta NV, et al. 2016. Restoring Cortical Control of Functional Movement in a Human with Quadriplegia. Nature. 533: 247-250.
[69] Fukuma R, Yanagisawa T, Saitoh Y, et al. 2016. Real-Time Control of a Neuroprosthetic Hand by Magnetoencephalographic Signals from Paralysed Patients. Scientific Reports. 6: 21781.
[70] Oxley TJ, Opie NL, John SE, et al. 2016. Minimally Invasive Endovascular Stent-Electrode Array for High-Fidelity, Chronic Recordings of Cortical Neural Activity. Nature Biotechnology. 34: 320-327.
[71] Fregni F, Freedman S, Pascual-Leone A. 2007. Recent Advances in the Treatment of Chronic Pain with Non-Invasive Brain Stimulation Techniques. Lancet Neurology. 6: 188-191.
[72] Fenton BW, Palmieri PA, Boggio P, Fanning J, Fregni F. 2009. A Preliminary Study of Transcranial Direct Current Stimulation for the Treatment of Refractory Chronic Pelvic Pain. Brain Stimulation. 2: 103-107.
[73] Nitsche MA, Boggio PS, Fregni F, Pascual-Leone A. 2009. Treatment of Depression with Transcranial Direct Current Stimulation (tDCS): A Review. Experimental Neurology. 219: 14-19.
[74] McIntire LK, McKinley RA, Goodyear C, Nelson J. 2014. A Comparison of the Effects of Transcranial Direct Current Stimulation and Caffeine on Vigilance and Cognitive Performance During Extended Wakefulness. Brain Stimulation. 7: 499-507.
[75] Hampstead BM, Briceno EM, Mascaro N, Mourdoukoutas A, Bikson M. 2016. Current Status of Transcranial Direct Current Stimulation in Posttraumatic Stress and Other Anxiety Disorders. Current Behavioral Neuroscience Reports. 3: 95-101.
[76] Nelson J, McKinley RA, Phillips C, et al. 2016. The Effects of Transcranial Direct Current Stimulation (tDCS) on Multitasking Throughput Capacity. Frontiers in Human Neuroscience. 10: 589.
[77] van’t Wout M, Mariano TY, Garnaat SL et al. 2016. Can Transcranial Direct Current Stimulation Augment Extinction of Conditioned Fear? Brain Stimulation. 9: 529-536.
[78] van’t Wout M, Longo SM, Reddy MK, et al. 2017. Transcranial Direct Current Stimulation May Modulate Extinction Memory in Posttraumatic Stress Disorder. Brain and Behavior.
[79] PowerWalk® Product Website. Accessed April 19, 2017: http://www.bionic-power.com/
[80] Ziezulewicz G. 2016. U.S. Army to Field-Test Wearable Power-Generation System in 2017. United Press International. Accessed April 19, 2017: http://www.upi.com/Defense-News/2016/10/27/US-Army-to-field-test-wearable-power-generation-system-in-2017/6231477580837/
[81] Donelan JM, Li Q, Naing V, et al. 2008. Biomechanical Energy Harvesting: Generating Electricity During Walking with Minimal User Effort. Science. 319: 807-810.
[82] Dementyev A, Kao H-L, Choi I, et al. Rovables: Miniature On-Body Robots as Mobile Wearables. Proceedings of the 29th Annual Symposium on User Interface Software and Technology. October, 2016: 111-120.
[83] Bui N, Meshot ER, Kim S, et al. 2016. Ultrabreathable and Protective Membranes with Sub-5 nm Carbon Nanotube Pores. Advanced Materials. 28: 5871-5877.
[84] Jia W, Bandodkar AJ, Valdes-Ramirez, et al. 2013. Electrochemical Tattoo Biosensors for Real-Time Noninvasive Lactate Monitoring in Human Perspiration. Analytical Chemistry. 85: 6553-6560.
[85] Bandodkar AJ, Molinnus D, Mirza O, et al. 2015. Epidermal Tattoo Potentiometric Sodium Sensors with Wireless Signal Transduction for Continuous Non-Invasive Sweat Monitoring. Biosensors and Bioelectronics. 54: 603-609.
[86] Munje RD, Muthukumar S, Selvam AP, Prasad S. 2015. Flexible Nanoporous Tunable Electrical Double Layer Biosensors for Sweat Diagnostics. Scientific Reports. 5: 14586.
[87] Gao W, Emaminejad S, Nyein HYY, et al. 2016. Fully Integrated Wearable Sensor Arrays for Multiplexed In Situ Perspiration Analysis. Nature. 529: 509-514.
[88] Glennon T, O’Quigley C, McCaul M, et al. 2016. ‘SWEATCH’: A Wearable Platform for Harvesting and Analysing Sweat Sodium Content. Electroanalysis. 28: 1283-1289.
[89] Seok S, Onal CD, Cho K-J. 2013. Meshworm: A Peristaltic Soft Robot With Antagonistic Nickel Titanium Coil Actuators. IEEE/ASME Transactions on Mechatronics. 18: 1485-1497.
[90] Wehner M, Truby RL, Fitzgerald DJ, et al. 2016. An Integrated Design and Fabrication Strategy for Entirely Soft, Autonomous Robots. Nature. 36 451-455.
[91] Shen H. 2016. The Soft Touch. Nature. 530: 24-26.
[92] Chu J. 2012. Soft Autonomous Robot Inches Along Like an Earthworm. MIT News. Accessed April 19, 2017: http://news.mit.edu/2012/autonomous-earthworm-robot-0810
[93] Jeong J-W, Yeo W-H, Akhtar A, et al. 2013. Materials and Optimized Designs for Human-Machine Interfaces via Epidermal Electronics. Advanced Materials. 25: 6839-6846.
[94] Kim HO. 2014. In-Vitro Stem Cell Derived Red Blood Cells for Transfusion: Are We There Yet? Yonsei Medical Journal. 55: 304-309.
[95] Shah SN, Gelderman MP, Lewis EMA, et al. 2016. Evaluation of Stem Cell-Derived Red Blood Cells as a Transfusion Product Using a Novel Animal Model. PLoS ONE. 11: 12.
[96] In-Man Trials of Manufactured Blood Within Two Years. 2015. NHS Blood and Transport. Accessed April 19, 2017: http://www.nhsbt.nhs.uk/news-and-media/news-articles/news_2015_06_25.asp
[97] Lee H, Choi TK, Lee YB, et al. 2016. A Graphene-Based Electrochemical Device with Thermoresponsive Microneedles for Diabetes Monitoring and Therapy. Nature Nanotechnology. 11: 566-572.
[98] Lee H, Song C, Hong YS, et al. 2017. Wearable/Disposable Sweat-Based Glucose Monitoring Device with Multistage Transdermal Drug Delivery Module. Science Advances. 3: 3.
[99] Huchon L, Badet L, Roy AC, et al. 2016. Grasping Objects by Former Amputees: The Visuo-Motor Control of Allografted Hands. Restorative Neurology and Neuroscience. 34: 615-633.
[100] Salminger S, Roche AD, Sturma A, Mayer JA, Aszmann OC. 2016. Hand Transplantation Versus Hand Prosthetics: Pros and Cons. Current Surgery Reports. 4: 8.
[101] Cetrulo CL Jr, Ng ZY, Winograd JM, Eberlin KR. 2017. The Advent of Vascularized Composite Allotransplantation. Clinics in Plastic Surgery. 44: 425-429.
[102] Shores JT, Malek V, Lee WPA, Brandacher G. 2017. Outcomes After Hand and Upper Extremity Transplantation. Journal of Materials Science: Materials in Medicine. 28: 72.
[103] Bowman DA, McMahan RP. 2007. Virtual Reality: How Much Immersion is Enough? IEEE Computer 36-43.
[104] Reger GM, Holloway KM, Candy C, et al. 2011. Effectiveness of Virtual Reality Exposure Therapy for Active Duty Soldiers in a Military Medical Health Clinic. Journal of Traumatic Stress. 24: 93-96.
[105] Rizzo A, Parsons TD, Lange B, et al. 2011. Virtual Reality Goes to War: A Brief Review of the Future of Military Behavioral Healthcare. Journal of Clinical Psychology in Medical Settings. 18: 176-187.
[106] Rizzo A, John B, Newman B, et al. 2013. Virtual Reality as a Tool for Delivering PTSD Exposure Therapy and Stress Resilience Training. Military Behavioral Health 1: 48-54.
[107] Hoffman HG, Meyer WJ III, Ramirez M, et al. 2014. Feasibility of Articulated Arm Mounted Oculus Rift Virtual Reality Goggle for Adjunctive Pain Control During Occupational Therapy in Pediatric Burn Patients. Cyberpsychology, Behavior, and Social Networking. 17: 397-401.
[108] Pallavicini F, Argenton L, Toniazzi N, Aceti L, Mantovani F. 2016. Virtual Reality Applications for Stress Management Training in the Military. Aerospace Medicine and Human Performance. 87: 1021-1030.
[109] XStat® Product Website. Accessed April 19, 2017: http://www.revmedx.com/xstat-dressing
[110] Mueller GR, Pineda TJ, Xie HX, et al. 2012. A Novel Sponge-Based Wound Stasis Dressing to Treat Lethal Noncompressible Hemorrhage. Journal of Trauma and Acute Care Surgery. 73: S134-139.
[111] Kragh JF Jr, Aden JK, Steinbaugh J, Bullard M, Dubick MA. 2015. Gauze vs XSTAT in Wound Packing for Hemorrhage Control. The American Journal of Emergency Medicine. 33: 974-976.
[112] Sims K, Montgomery HR, Dituro P, et al. 2016. Management of External Hemorrhage in Tactical Combat Casualty Care: The Adjunctive Use of XStat™ Compressed Hemostatic Sponges: TCCC Guidelines Change 15-03. Journal of Special Operations Medicine. 16: 19-28.
[113] Wiseman E, 2016. Human Optimization Research: International Activity. Prepared for: Keith Niall. National Research Council of Canada (STI-EW-060) and Defence Research and Development Canada (IR65051601).
[114] NASA Technology Readiness Levels. Accessed April 20, 2017: https://esto.nasa.gov/files/trl_definitions.pdf
[115] Singer PW. 2010. The Ethics of Killer Applications: Why Is It So Hard To Talk About Morality When It Comes to New Military Technology? Journal of Military Ethics. 9: 299-312.
[116] Lin P, Mehlman MJ. Abney K. 2013. Enhanced Warfighters: Risk, Ethics, and Policy. Prepared for: The Greenwall Foundation.
[117] Thorpe JB, Girling KD, Auger A. 2017. A Framework to Assess the Military Ethics of Emerging Technologies. In Submission to Journal of Military Ethics.
[118] Casebeer WD. Ethics and the Biologized Battlefield: Moral Issues in 21st-Century Conflict. In: Bio-Inspired Innovation and National Security. Eds: Robert E. Armstrong, Mark D. Drapeau, Cheryl A. Loeb, and James J. Valdes. Washington, D.C.: National Defense University Press. 2010; p. 293-303.
[119] Michaud-Shields M. 2014. Personal Augmentation – The Ethics and Operational Considerations of Personal Augmentation in Military Operations. Canadian Military Journal. 15: 24-33.
[120] Shunk D. 2015. Ethics and the Enhanced Soldier of the Near Future. Military Review Jan-Feb: 91-98.
[121] Chameau J-L, Ballhaus WF. Lin HS. (Eds). 2014. Emerging and Readily Available Technologies and National Security – A Framework for Addressing Ethical, Legal, and Societal Issues. Washington, D.C.: The National Academies Press.
[122] Multi-Domain Battle: Combined Arms for the 21st Century White Paper. February 24, 2017. Accessed April 21, 2017: http://www.tradoc.army.mil/MultiDomainBattle/docs/MDB_WhitePaper.pdf
End Note
[i] The HE technologies presented here were identified through searches of the primary literature and opportunistic sampling of science news media. This list is by no means complete, and is presented here merely as a small sample of HE technologies that the U.S. military may have at its disposal in the future, and to illustrate how HE technologies may contribute to soldier resilience.
About the Author(s)

Joelle Thorpe received her Master of Science degree in Biology from Queen’s University in Kingston, Ontario, Canada in 2009, and earned her doctorate in Psychology, Neuroscience and Behaviour from McMaster University in Hamilton, Ontario, Canada in 2013. Her research interests include neuroendocrinology, stress physiology, and the influence of psychological stress on reproduction. During her time as a Clinical Research Associate from 2014 to 2016, Dr. Thorpe developed an interest in ethics, and sat as a board member on the Queen’s University & Affiliated Teaching Hospitals Health Sciences Research Ethics Board. She is currently a Mitacs Canadian Science Policy Fellow, working in the Office of the Chief Scientist at Defence Research and Development Canada. Here, Dr. Thorpe is part of a team investigating the potential ethical issues and policy implications associated with emerging human enhancement technology use in the military.

Dr. Kimberly Girling is a Mitacs Canadian Science Policy Fellow with Defence Research and Development Canada in the Office of the Chief Scientist. Her work aims to identify ethical and policy challenges to the implementation of human performance enhancement technologies within the Canadian Armed Forces. Dr. Girling earned her PhD in Neuroscience from the University of British Columbia developing preventative therapeutics for Huntington’s disease, a genetic neurodegenerative disease. During her PhD work, Kimberly developed a passion for health and science policy, leading her to become involved in several initiatives and projects across Canada, including sitting as a board member for the Neglected Global Diseases Initiative, working on a three year project for the Status of Women Canada on women in science, working closely with the Canadian Drug Policy Coalition, and initiating a cross-Canada survey on substance use and harm reduction. For several years, Kimberly also served as the President of the Student Biotechnology Network, a BC-wide organization that helps students develop career paths in life science and biotechnology through education about career opportunities and connection with industry leaders.

Alain Auger received a Ph.D. degree in Linguistics from Université de Neuchâtel in Switzerland in 1997. He has developed new methods to capture and fuse semantic information in electronic texts. His main research interests include knowledge capture and representation, terminology extraction, text and audio mining, ontology engineering, machine translation, automated document summarization and automated document classification.
He joined Defence Research and Development Canada (DRDC) as a Defence Scientist in 2003 and delivered several innovative capabilities to the Intelligence community. Dr. Auger was deployed as the Scientific Advisor to General Jonathan Vance in 2009-2010 during Op ATHENA in Afghanistan. He led TTCP panel JSA TP9 (2013-2017) which raised TTCP Groups’ awareness of emerging and potentially disruptive technologies.
He is currently leading DRDC's Science and Technology Outlook function within the Office of the Chief Scientist with the mandate to identify and assess the potential impact of emerging technologies on Defence and National Security to support DRDC's S&T program formulation and investments.
Comments
The fact is as the world approaches significant global crisis, genocide will continue to be considered by some leaders as an ethical solution for nation states. Denial and Rationalization of genocide in Islamic states. This is already taking place and largely ignored in Islamic states already suffering severity from population growth and a climate and topography that can not support it.
The treatment of non-Muslim and even dissenting Muslim peoples by the Islamic State and multiple other Islamic nations is probably just an emerging facet of the problems in part described by the authors.
Even when you put the Israeli versus the Arab (Islamic Iran threatens to use a nuclear bomb delivered by missiles in 11 years. just hyperbole?) state and Palestinian conflicts in perspective the 1967 war was Nasser's solution to dissolve the Jewish Homeland and annihilate the Jews. By 1967, the Arab and other Islamic states and disgorged themselves of their Jewish populations, they resettled in Israel but not as refugees and they arrived in numbers equal to the numbers claimed by the UN to equal their clients, Palestinians. Nasser's military initiatives caused the UN peace keepers to beat feet and the Israeli's to preempt Nasser's final solution. With the continued trend to justify or rationalize antisemitism in the west and pretend it is merely an anti-Zionist settler gesture the fact is all assumptions being made in that regard are false positives. It serves the Islamists well and by removing the issue of Jewish versus Muslim identities, modern state versus sharia law state it further distracts and even minimizes the ongoing persecution and genocide of other non-Muslim groups.
Ethical?
How can we write of ethics if we exclude these facts pertinent to genocide, from any meaningful debate?