Providing Basic Sanitation: A Means to Achieving the Military’s Strategic Objectives During Stability Operations
Adam Brady, Andrew Pfluger, Erin Mauldin, and Jeffrey Starke
Introduction
As indicated in the 2010 Quadrennial Defense Review, America’s Armed Forces need to “rebalance” to face future threats.1 This thought is reiterated in the 2010 National Security Strategy, which specifically states that “we will continue to rebalance our military capabilities to excel at counterterrorism, counterinsurgency, stability operations, and meeting increasingly sophisticated security threats, while ensuring our force is ready to address a full range of military operations”.2 In the recent Iraq and Afghanistan conflicts, the Army has continuously executed stability operations while simultaneously balancing the execution of counterinsurgency operations. Indeed, the Department of Defense has stated that stability operations should be given similar priority for training and execution to combat operations.3 The current Chief of Staff, General Odierno, recently framed these thoughts by stating that the US Army has three roles to play: prevent, shape, and win.4 The objectives of stability operations are closely related to prevent and shape roles. The provision of basic services, to include the focus of this paper – basic sanitation – are key components to successful stability operations and most closely align with General Odierno’s definition of our shaping role. Providing basic services allows the US military to enable our allies by improving health and building their capacity to effectively govern and meet the needs of their people.
The conduct of stability operations within the U.S. Army is primarily governed by Army Doctrinal Reference Publication (ADRP) 3-07: Stability. This document directly charges the Army with restoring essential services that provide for the livelihood and well-being of local citizens and the state. Reconstruction of critical infrastructure and basic services, such as roads, electric power lines, sewers, and health related public services, such as sanitation and clean water, are key components of stability operations.5 Due to the nature of military operations, ADRP 3-07 places heavy emphasis on providing a secure environment for government agencies, non-governmental organizations (NGOs), international governmental organizations (IGOs), and local groups to provide assistance. The military is charged with conducting stability operations within a whole-of-government construct, which includes working with aid-providing agencies such as the United States Agency for International Development (USAID). The goal of this approach is to ensure all facets of the government, both military and civilian, complement each other and are seamlessly integrated.6 This unity of effort is now required in the joint doctrine of the U.S. military.7
The emphasis on providing security, coupled with the decentralized nature of Mission Command, has precluded a detailed discussion on the best methods of providing basic services to a local population within current Army doctrine. A gap exists between civilian development and military organizations when there is a clear need for the establishment of basic services, but a prolonged period of security risk prevents non-military groups from operating in an area. To effectively bridge this gap and complete the mission, the Army must develop an understanding of how to provide the most basic services while simultaneously improving the security situation.
While the military has more than a decade of experience addressing infrastructure construction in Iraq and Afghanistan, it still has much to learn concerning the development of effective, sustainable solutions for basic services. Though the US Department of State, through USAID, is the agency primarily responsible for foreign development operations, they are not always able to operate – especially during periods of increased security risk. This paper makes the case that the military should focus on training Soldiers and small unit leaders to be competent in assessing and providing basic services that are in line with USAID priorities and methods. While the need exists in several public service areas, we focus on sanitation because it one of the most important, yet most overlooked topics, both in the areas the US has been involved and in the military. Improving basic sanitation offers a unique opportunity for the military to engage and connect with the local people, improve their health and well-being, and foster a sense of trust.
The Need for Basic Sanitation in Developing Countries
Developing countries throughout the world – where the military predominantly deploys – face a multitude of health-related issues due to a lack of adequate basic sanitation and the scarcity of clean water. These health-related issues are not new problems. In 1998, safe drinking water was reported to be unavailable to over 1 billion people in developing countries, and resulted in the death of greater than 400 children under the age of five per hour.8 Recent statistics indicate that, despite many unilateral efforts over the last 15 years, the number of those without clean water has remained approximately the same.9 The statistics concerning basic sanitation, which is defined as the “lowest-cost technology ensuring hygienic excreta and sullage disposal and a clean and healthful living environment both at home and in the neighborhood of users”, are much worse.10 Approximately 2.6 billion people, just less than 40% of the world’s population, do not have access to basic sanitation services and are at increased risk of contracting waterborne illness.11 Water related illnesses caused by unclean water and poor sanitation are responsible for the majority of sickness in developing countries. Afghanistan, for example, suffers the highest child mortality rate in the world and has some of the lowest coverage for basic water and sanitation infrastructure. The World Health Organization (WHO) estimates that 257 of every 1000 children under age five die in Afghanistan – the highest rate worldwide. The highest portion of deaths (28.9%) is attributable to diarrhea and other unclean water and poor sanitation-related diseases.12 Indeed, as of 2010, approximately 90% of the population did not have access to basic sanitation.13 The United Nations recently stated that more individuals in the developing world have access to cell phones than basic sanitation services.14 A study conducted by Bartram et al (2005) found that poor sanitation and unclean water supplies affect more people than war, terrorism, and weapons of mass destruction combined.15 WHO reports that more than 3.4 million people die from poor sanitation and water related disease per year, making it the leading cause of disease and death worldwide.16
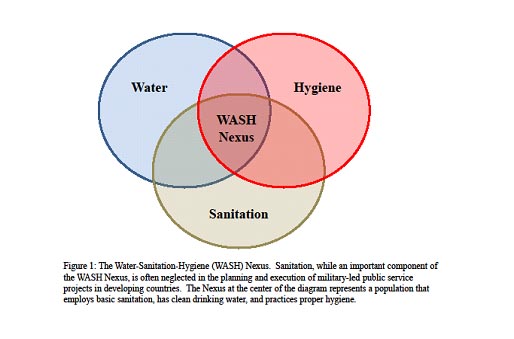
Clean water, basic sanitation, and proper hygiene are inextricably tied and are essential to sustained human health. Poor sanitation practices often leads to unclean water, as human feces are often dumped around or near local water sources. Consumption of unclean water, or a failure to perform basic hygiene, such as washing hands after defecation, leads to the fecal-oral route of transmission, which can in turn cause health issues such as diarrhea. Figure 1 indicates how water, sanitation, and hygiene (WASH) intersect. A healthy population that exists in the “WASH Nexus” is one that employs basic sanitation, consumes clean drinking water, and practices proper hygiene.
The need for increased sanitation throughout the developing world has been recognized by prominent international organizations such as the UN and WHO. Each of these organizations has issued guidelines to assist other governmental and non-governmental organizations in alleviating water and sanitation problems in developing countries. The United Nations’ Millennium Development Goals (MDG) are a challenge for all countries to reduce global poverty, hunger, disease, gender inequality, and environmental degradation by 2015. Included in this challenge are provisions for clean water, water treatment, and sanitation. Specifically, MDG Target 7c calls for the reduction of those without access to safe drinking water and basic sanitation by half by the year 2015.17 Additionally, WHO established guidelines for drinking water standards based on assessments of the health risks from microbial, chemical, and physical constituents of drinking water, as well as researching and establishing standards for sanitation and latrines.18 The US Department of State and USAID have adopted the MDGs as the way ahead for development throughout the world. To implement a unity of effort across the spectrum of agencies and organizations, the US military should also establish MDGs as stability operation objectives. Additionally guidelines from WHO should be considered when establishing appropriate metrics of success in order to standardize assessments across organizations.
While preventing open defecation and safeguarding drinking water may seem like common sense to those in most developed countries, the lack of formal education in developing areas, such as rural Afghanistan, has made many residents ignorant to the threats of water-related illness exacerbated by poor basic sanitation. An example of improper education, and the opportunity that exists with basic sanitation education, was observed by the author in Al Qa’im, Iraq in February 2004.19 US Army Soldiers from the 3d Armored Cavalry Regiment and Iraqi Soldiers were co-located at the Iraqi-Syrian Border Control Point (BCP) with the mission of controlling people and goods travelling between Iraq and Syria. Iraqi Soldiers did not have a location to defecate in the BCP, and to prevent open defecation, US Soldiers constructed a series of wooden outhouses for the Iraqis and gave them instructions on how they should be maintained. The Iraqi Soldiers, however, had little knowledge of the importance of properly maintaining such an outhouse or the health risks associated with amassing large quantities of fecal matter. Due to the Iraqis failure to properly dispose of the fecal matter, it accumulated to the point where the outhouse needed to be burned (see Figure 2). Education by the US Soldiers at the BCP could have prevented the outhouse from being destroyed, potentially increased the health of the Iraqi Soldiers (by decreasing their exposure to pathogen-laden feces), and fostered an environment of partnership and trust.

Picture 1

Picture 2

Picture 3
Pictures of an outhouse built by American Soldiers for Iraqis at the Al Qa’im, Iraq border checkpoint (circa 2004). Pictures 1 and 2 show improperly maintained outhouses with amassed human feces. The outhouses became unusable and needed to be burned (Picture 3).
How the US has Addressed Sanitation in Afghanistan
In recent conflicts and security engagements, the US government has devoted resources to, and involved several organizations and agencies in, addressing sanitation and water issues as a part of stability operations. While USAID and State Department organizations have been the primary agencies for sanitation development projects, the Department of Defense has found itself playing a significant role in funding and carrying out those projects. The reality of security situations in Afghanistan and Iraq prevented many government agencies from being able to establish a presence due to a lack of security.
In Afghanistan, USAID, the Department of Defense, and the State Department have all been involved in sanitation development projects – some in conjunction with each other and some in conjunction with the Afghan government, or both.20 For example, USAID’s Sustainable Water Supply and Sanitation (SWSS) program has partnered with non-governmental organizations (NGOs) to implement Community-Led Total Sanitation21,22 (CLTS) and hygiene education programs, in addition to providing technological assistance. The DOD’s Commander Emergency Response Program (CERP) funded over 1,178 water, sanitation, and hygiene related projects in Afghanistan between 2006 and 2010.23 Nevertheless, considerable sanitation issues remain today, as approximately 90% of the population still practice open defecation and 75% drink contaminated water on a daily basis.24 Progress in basic sanitation has been achieved where community involvement, localized attention, long-term planning, and cross-agency and/or cross-government cooperation have come together with consistent funding, resulting in sustainable implementation of technology. To-date, sanitation projects have not generally worked when they were initiated by units on short deployment cycles that placed a high value on inadequate metrics, such as dollars spent, rather than on a long-term investment in a community. Sanitation-related progress has also been significantly hampered by a lack of unity of effort and coordination between the governments and agencies involved (between the US government agencies themselves, and between those agencies and the Afghan government), a short-term focus, and a lack of continuity in terms of mission objectives and operational-level leadership.
Running from 2009-2012, USAID’s SWSS program found success balancing the prevalent “hardware” approach to sanitation problems (the implementation of technological solutions) with an emphasis on “software” (providing hygiene education and changing attitudes of communities towards sanitation). However, USAID’s water-related projects appeared to suffer from gaps in performance management and monitoring efforts, and a lack of coordination with the DOD and the State Department in Afghanistan working on similar projects.25 Using CLTS, the formation of Family Health Action Groups, hygiene education, and the construction and training on maintenance of water pumps and latrines, the SWSS program has made much progress. SWSS trained community workers have “triggered”26 1,031 communities in Afghanistan, resulting in 611 Open Defecation Free communities, 42,129 improved latrines, and an estimated 574,091 beneficiaries of hygiene education programs across six provinces.27
To date, the Department of Defense’s role in sanitation development has mainly been through CERP, while the State Department controls Provincial Reconstruction Teams (PRTs) composed of civilian and military experts working together. CERP was designed to enable local military leaders in Afghanistan and Iraq to fund and implement reconstruction projects and services that could be sustained by the community or the local government as a means of ensuring security in the short-term and stability in the long-term. PRTs are intended to help rebuild host government capacity in areas where conflict still poses a threat and in areas where the international community and NGOs are unable or unwilling to operate.28 In 2010-2011 alone, PRTs and local commanders using CERP implemented 187 water, sanitation, and hygiene education related projects, spending $12,513,039 of the total $901,455,648 spent on CERP projects (or about 1.3%).29 Unfortunately, DOD and State Department projects have produced mixed results, and the beneficial infrastructure initiatives have been undermined in some cases by negative attitudes towards PRTs and CERP.30
Shifting Focus: How we can Achieve Stability Objectives through Basic Sanitation
As indicated, developing solutions to infrastructure problems, especially sanitation, requires a comprehensive approach. Additionally, stability operations are ideally conducted in coordination with other governmental and non-governmental organizations. To create the conditions for success, a unity of effort must be realized across the diverse organizations involved. This unity, as defined by Joint Publication 1, is “the coordination and cooperation toward common objectives, even if the participants are not necessarily part of the same command or organization.”31 According to ADRP 3-07, this unity of effort is reached through the following approaches: whole-of-government and comprehensive. The term “whole-of-government approach” describes unity of effort within the departments and agencies of the US government.32 ADRP 3-07 defines “comprehensive approach” as one that integrates the US government and “intergovernmental organizations, non-governmental organizations, multinational partners, and private sector entities to achieve a unity of effort towards a shared goal.”33
For military units, this unity of effort plays a direct role in planning and executing stability operations. PRTs are the most visible manifestation of this unity of effort. Based on the “whole-of-government” approach, PRTs have the inherent ability to create a unity of effort between government departments and agencies.34 This capability, if properly utilized, ensures military units will recognize the potential impacts of any actions that they take. A PRT also has the ability to create a comprehensive approach to stability when it coordinates with other organizations outside of the US government.
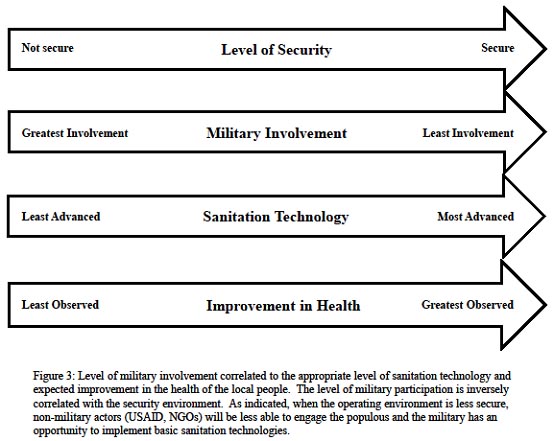
The availability of PRTs to plan and organize the implementation of public service projects, however, can be limited based on their availability and the security of the local operating environment. Figure 3 indicates that the level of non-PRT military involvement, most specifically ground combat units, in the provision of basic services such as sanitation is strongly influenced by the security environment. In areas that are not secure, the military will be most greatly involved in reestablishing services as part of stability operations, simply because the military has the greatest access. At the same time, providing basic services, such as sanitation, is not the military’s primary mission and therefore the level of sanitation technology that the military should be expected to provide is not advanced. The military should simply begin to set the conditions to improve human health by increasing the level of sanitation awareness and facilitating the creation of basic sanitation infrastructure – the first steps of CLTS. As the security situation improves, there will be increased opportunity for PRTs and aid organizations, such as USAID, to implement more advanced sanitation technologies and practices. When the security situation is most stable, the military should be least involved, and aid organizations should have the ability to operate virtually unimpeded to develop more extensive solutions to the sanitation problem. The Sudanese Refugee case study (Table 1) shows a situation a scenario similar to ones that that US military may face and where an approach similar to CLTS was used to assist the local populace improve basic sanitation infrastructure.
The relative success of the CLTS approach implemented by USAID in Afghanistan indicates that such an approach can be implemented by military units in deployed environments when the security situation dictates that external assistance is unavailable. CLTS would set the stage for follow-on assistance by USAID and NGOs, and would therefore also be the most appropriate approach to create the required long-term unity of effort. Integration of CLTS would ensure a seamless transition of any sanitation effort conducted by a military unit to USAID personnel when the security situation allows.
An additional benefit to military units successfully implementing CLTS is improved relations with the local population, which can be provided by a tangible improvement in their health and well-being. More specifically, CLTS can allow military units the ability to gain and maintain a relationship with the local population, increase their legitimacy in the eyes of the population, and further the overall stability goals. As the security in the area improves, agencies such as USAID or NGOs, can build upon the foundational work that the military provided and continue to improve relationships while simultaneously improving basic sanitation services.
Sudanese Refugee Case Study.35 This case study involves the construction of household pit latrines at the Farchana camp for Sudanese refugees in Chad. Secours Catholique Développement (SECADEV), a Chadian NGO, needed a long-term solution for fecal management that would be sustainable and applicable to the unique conditions found in the camp. The Farchana camp, home to 5,560 refugee families, is located in the deserts of eastern Chad. This environment, coupled with the unknown future timeframe for the camp’s existence, created significant challenges that had to be overcome. SECADEV, following the recommendation of another NGO, created single family pit latrines that consisted of two pits. One of the pits is to be used at a time. When the first pit is full, it will be covered to minimize the contact with raw sewage while allowing for limited treatment to take place prior to emptying. This system, without emptying the pits, is expected to be functional for four to six years. By emptying the pits, the system has the potential to last for the duration of the camp’s existence. At an estimated cost of €495, it represents a small-scale sanitation project that can be executed by military units.
Challenges with Integrating Sanitation
There are several challenges faced by the military in creating a better understanding of sanitation issues and solutions. On an internal, tactical level, sanitation field craft training is insufficient and the unit Field Sanitation Team concept does not support current operations and the fluid nature of the battlefield.36 Field Sanitation Teams assigned on the company level are hard-pressed to respond to all of a units’ hygiene and sanitation needs, and cannot by themselves compensate for a lack of training in sanitation field craft best practices. Creating an outward focus on providing basic sanitation to others will likely allow the military to re-focus on its own field hygiene and sanitation practices, which can help reduce the incidence of disease non-battle injury (DNBI).
Further, using sanitation as an engagement tool during stability operations must overcome several difficulties: sanitation projects are not effective unless they are nested within a coherent operational and strategic vision, and the military must coordinate better with other government agencies and NGOs with expertise in sanitation.
The effectiveness of CERP funded projects, and the work of PRTs, in promoting stabilization and security in this arena has been questionable in Iraq and Afghanistan. The ineffectiveness can be contributed to an emphasis on creating short-term results within the time frame of short deployments, and because the projects often focused on socio-economic solutions to political and corruption issues.37 Many Afghans, for example, hold negative perceptions of CERP and PRT projects, feeling that many of the projects are insufficient, unevenly distributed, and associated with extensive corruption.38 Projects where commanders felt compelled to spend large amounts of money to produce short-term tactical results were ultimately destabilizing by generating competition and conflict over aid resources and by tending to strengthen already dominant groups entrenched in the corrupt political system.39 The stigmas of CERP and PRTs that stem from the perceived corruption and from the lack of continuity undermine advances made on the small-scale, making it difficult for there to be long-term stability gains, even for projects that may otherwise have been appropriate in a specific area. Further, a greater effort to coordinate the actions of government agencies involved in promoting sanitation projects (foremost being USAID, the State Department, and DOD) is needed to avoid repeating mistakes, undermining long-term projects, and to develop better measures of progress.40
Nevertheless, while security and stability may not have been directly improved, the projects were valuable in terms of development in areas where basic needs keep people in poverty.41 Understanding how to approach basic infrastructure issues within a community is critically important. The lessons coming from the management of some sanitation projects and the overall mixed results of CERP and PRTs provide an opportunity to improve the Army’s approach to those infrastructure issues. Effective local development empowers communities, which has been essential in Afghanistan, where “everything of importance… happens in the village.”42 Incorporating into training the fundamentals of sanitation and water considerations improves military teams’ approaches to improving infrastructure, and enables them to make lasting, positive change in areas where USAID and NGOs cannot go. Sanitation progress has the possibility of creating an immediate, but also lasting, impact within communities. For such sanitation projects to have that lasting stability influence, they must be matched with a coherency on the operational level in terms of the political structures that the military and U.S. Government choose to strengthen and support.
Finally, on the strategic level, the pursuit of sanitation solutions as a part of empowering partners and building their capacity to govern is not in and of itself a strategy and is by no means applicable in all situations. With the shifting of focus of many areas of foreign policy on the Pacific region and in engaging China, addressing sanitation issues will not be the primary military solution. However, putting sanitation on the strategic radar is important in most regions the military is engaged. All of the regional combat commands have important regional security, stability, humanitarian, disaster relief, and engagement objectives.43 Sanitation issues are directly tied to those missions, but the challenge will be convincing strategists and policy makers that in an era of fiscal constraints, sanitation awareness and focus is a worthwhile, cost-effective, and security-vital investment.
Opportunities to Integrate Sanitation
The integration of sanitation into military operations provides many opportunities to improve the success of any military operation. These opportunities include decreasing disease, creating an immediate and visible impact in the local area, providing a foundation to foster future unity of effort among all stakeholders, and directly supporting of the “Prevent” and “Shape” concepts espoused by the US Army Chief of Staff.
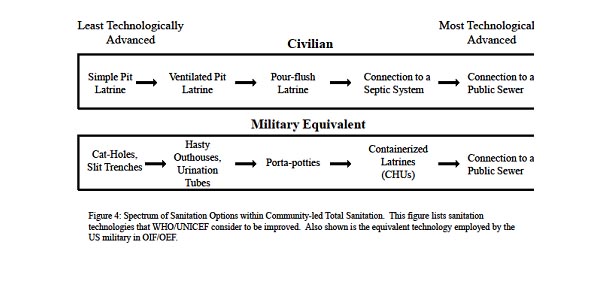
Providing basic sanitation is a proven method to decrease the prevalence of disease in developing country communities. The technology required to implement this level of sanitation is fairly simple. By having Soldiers and leaders trained in the techniques and procedures of sanitation, individual units can directly improve the quality of life for the local community. Figure 4 indicates the parallels between civilian sanitation technologies and their military equivalents. As shown, most basic sanitation technologies are ones that members of the military are already familiar with. Educating small unit leaders on how to implement aspects of CLTS, such as triggering, providing basic sanitation education, and construction of latrines (simple pit and ventilated pit), can significantly improve the level of sanitation in a community and decrease the prevalence of disease.
The implementation of these technologies also provides an immediate and visible impact on the surrounding community. In the short-term, highly visible useful projects helps to increase the legitimacy of the military unit operating in the area. By demonstrating an intention to support the local population and improve their quality of life, the presence of US military units may be welcomed, if not sought out. Sanitation projects, provided they are sustainable and functional, can also improve the long-term legitimacy and capacity of the local government.
In addition, sanitation projects provide a common foundation for military units and other agencies and organizations to improve relations. These relatively simple projects have the potential to lead to more integrated and complicated operations between these seemingly disparate organizations, thereby increasing unity of effort.
Conclusions and Recommendations
The US military will continue to conduct stability operations for the foreseeable future. The ability to provide services, including basic sanitation, is essential to the success of any stability operation. While the military has more than a decade of experience conducting stability operations, it still has much to learn about the development of basic infrastructure, to include the provision of basic sanitation and clean water. The lead and most experienced agency for development in the U.S. government, USAID, does not have the capability to operate in unsecure and hostile environments. The time gap between the conduct of military operations and reaching a level of security sufficient for external aid agencies and NGOs to operate requires the military be prepared to execute the development roles normally reserved for those groups. This gap in the provision of basic sanitation, when combined with the requirement for unity of effort across all entities, government and non-government, necessitates that the military tie into current USAID programs – the most implementable being CLTS. CLTS will allow military units to provide an essential service and create an immediate impact in a local area, while fostering trust within the local population and facilitating the future transition of these critical projects to other organizations when the security situation improves.
The views expressed in this article are those of the author(s) and do not reflect the official policy or position of the Department of the Army, the United States Military Academy, Department of Defense, or the U.S. Government.
End Notes
1 U.S. Department of Defense. Quadrennial Defense Review. February 2010, iii. Available from http://www.defense.gov/qdr/images/QDR_as_of_12Feb10_1000.pdf . Accessed 01 April 2013.
2 White House. National Security Strategy, 2010 (Washington, D.C., May 2010), 14.
3 U.S. Department of Defense. "Department of Defense Instruction #3000.05" (Washington, D.C., September 2009).
4 Association of the United States Army. “Odierno: Army has three principle roles – ‘Prevent, Shape, Win’.” Available from http://www.ausa.org/publications/ausanews/specialreports/2012/03/Pages/OdiernoArmyhasthreeprincipleroles%E2%80%93%E2%80%98Prevent,Shape,Win%E2%80%99.aspx. Accessed 01 April 2013.
5 U.S. Department of the Army. Army Doctrinal Reference Publication 3-07: Stability Operations (Washington, D.C.: Department of Defense, 2011).
6 National Security Strategy, 2010.
7 U.S. Department of Defense. Joint Publication 1: Doctrine for the Armed Forces of the United States (Washington D.C., 2011), II-7.
8 Gadgil, A. 1998. Drinking water in developing countries. Annu. Rev. Energy Environ. 23:253–86.
9 World Health Organization. “Health through safe drinking water and basic sanitation”, Available from: http://www.who.int/water_sanitation_health/mdg1/en/. Accessed: 01 April 2013
10 Ibid.
11 United Nations Development Programme (UNEP), 2010. What will it take to achieve the Millennium Development Goals? – An International Assessment. United Nations Development Programme, New York, New York.
12 From the 2008 WHO Global Health Observatory Database at http://apps.who.int/ghodata/#. Accessed: 28 March 2011.
13 United States Agency for International Development Afghanistan. Community-Led Total Sanitation. 15 August 2010. http://afghanistan.usaid.gov/en/USAID/Article/1348/Communityled_Total_Sanitation. Accessed: 20 March 2013.
14 UN News Centre, 2013. Deputy UN chief calls for urgent action to tackle global sanitation crisis. Available from: http://www.un.org/apps/news/story.asp?NewsID=44452. Accessed: 23 May 2013
15 Bartram, J., Lewis, K., Lenton, R., Wright, A., 2005. Focusing on improved water and sanitation for health. Lancet: 365(9461):810-812.
16 Berman, J., 2009. WHO: Waterborne Disease is World’s Leading Killer. Available from: http://www.voanews.com/content/a-13-2005-03-17-voa34-67381152/274768.html
17 United Nations, “Millennium Development Goal 7: Ensure Environmental Sustainability” Available from: http://www.un.org/millenniumgoals/environ.shtml. Accessed: 01 April 2013.
18 World Health Organization, 2008. Guidelines for Drinking-water Quality, Third Edition Incorporating the First and Second Addenda. Volume 1: Recommendations. World Health Organization, Geneva. Available from: http://www.who.int/water_sanitation_health/dwq/gdwq3rev/en/. Accessed: 26 Feb 2013.
19 MAJ Andrew Pfluger was deployed to Al Qa’im in the Al Anbar Province of Iraq from April 2003-March 2004.
20 USAID. Community-Led Total Sanitation.
21 Community Led Total Sanitation “works by engaging whole communities in examining and acknowledging the extent and shamefulness of open defecation, its importance in the transmission of diarrheal diseases, and the costs of such diseases to well-being and household finances.” The longer term success achieved by CLTS is due to the fact that it motivates communities to resolve sanitation issues through education on its importance. It is achieved within the scope of a communitiy’s resources (USAID SWSS 2012).
22 United States Agency for International Development. Afghan Sustainable Water Supply and Sanitation (SWSS) Project: Sustainable Health Outcomes Unit Project Final Report. 20 September 2012. http://sanitationupdates.files.wordpress.com/2012/12/afghanistan-swss2012.pdf. Accessed: 20 March 2013.
23 United States Government Accountability Office. Afghanistan Development. November 2010. http://www.gao.gov/assets/320/312291.html . Accessed: 20 Mar 2013 (GAO-11-138).
24 Tetra Tech. USAID Afghanistan Sustainable Water Supply and Sanitation. 2012. http://www.tetratech.com/projects/usaid-afghanistan-sustainable-water-supply-and-sanitation.html. Accessed: 20 March 2013.
25 GAO. Afghanistan Development.
26 “Triggering” is the term applied to the introduction of CLTS to communities by the NGO facilitators.
27 USAID. Afghan SWSS, 2-3.
28 Nima Abbaszadeh et. al. “Provincial Reconstruction Teams: Lessons and Recommendations.” Princeton University Woodrow Wilson School of Public & International Affairs. January 2008. http://wws.princeton.edu/research/pwreports_f07/wws591b.pdf. Accessed 20 March 2013, 5.
29 GAO. Afghanistan Development.
30 Paul Fishstein and Andrew Wilder. “Winning Hearts and Minds? Examining the Relationship between Aid and Security in Afghanistan.” Tufts University Feinstein International Center, January 2012. http://sites.tufts.edu/feinstein/files/2012/01/WinningHearts-Final.pdf. Accessed: 30 March 2013, 41.
31 Joint Publication 1.
32 ADRP 3-07, 1-15 to 1-21.
33 ADRP 3-07, 1-21.
34 Center for Army Lessons Learned, “Afghanistan PRT Handbook,” http://usacac.army.mil/cac2/call/docs/11-16/11-16.pdf (accessed March 26, 2013), p. 5.
35 Sustainable Sanitation Alliance, “Case study of sustainable sanitation projects,” http://www.susana.org/docs_ccbk/susana_download/2-1623-casestudybookafrica2012.pdf (accessed March 26, 2013), p. 4-1 to 4-6.
36 LTC Timorthy Bosetti and CPT Davin Bridges. “The Unit Field Sanitation Team: A Square Peg in a Round Hole.” U.S. Army Medical Department Journal, April-June 2009, 31.
37 Fishstein and Wilder, 57.
38 Ibid., 41.
39 Ibid., 44.
40 GAO, Afghanistan Development.
41 Fishstein and Wilder, 71.
42 Don Rector of the Army’s Human Terrain System in “Afghan Local Police-An Afghan Solution to an Afghan Problem.” Army Irregular Warfare Cell Newsletter, 20 January 2012. http://usacac.army.mil/ cac2/AIWFC/repository/Army%20IW%20Fusion%20Cell%20Newsletter%20JAN12.pdf (accessed 31 March 2013), 2.
43 See mission statements at http://www.centcom.mil/en/about-centcom/our-mission/, http://www.africom.mil/about-the-command/cornerstones/support-humanitarian-and-disaster-relief, http://www.southcom.mil/ourmissions/Pages/Our-Missions.aspx, and http://www.pacom.mil/about-uspacom/2013-uspacom-strategy.shtml.
About the Author(s)
Comments
Thanks for the comment. I know that ESEOs have their hands full with the units they support and partner nations. The issue with ESEOs, based on my limited experience with them during deployments, is the small number that are available. My BDE had 8+ FOBs and COPs during my last deployment. The BDE MED team did not have the capability to provide significant support to individual units spread out throughout the battlespace. Given the possibility of more austere living conditions in future military operations, military units must become more versed in providing their own sanitation facilities. The argument we are making is that small units may have an opportunity to provide these sanitation options to the local area that they are interacting with, as well. This will provide an additional "positive outcome" for improving the sanitation training within small units.
Very interesting article. As ESEOs this is a challenge that we face constantly not only among partner nation forces but among our own military as well. This also, I think, highlights the need to engage with the public health team available to commanders at all levels, including the BCT, Division, SFG, and EAB assets such as Preventive Medicine detachments and MMBs. The officers and senior NCOs assigned to these elements recieve specific training in how to develop sanitation strategies in field and disaster response evnironments.
There are literailly hundreds of references from WEDC, WELL, Lifewater CA on how to develop and implement strategies for sanitation, but may I also suggest the hesperian reference "A community guide to environmental health" http://store.hesperian.org/HB/prod/B160.html which provides excellent tools to work with host nation personnel.
Davidbfpo,
Thanks for the comment. You bring up a good point, though I don't think it's one that you meant. The Lifesaversystem that you mention, and many others like it, are focused on providing clean water through filtration without doing anything about the sanitation aspect of the problem. The focus of this paper was to look at actually dealing with the sanitation problem(s) that military units may see upon arrival in a humanitarian assistance/disaster relief environment or during stability operation.
While it looks like impressive technology (based on checking out the website you mentioned), I would also question the sustainability of using it. At ~$250 per jerry can, it is an expensive option that will have to be replaced with some regularity. That replacement, if reliable/practical shipping is even available, must come from a company in the US. This creates 2nd and 3rd order effects with regards to the local economy, the efficient use of funds, and ability of a solution to be successful upon the removal of outside assistance.
I think this may be a good option for someone during a holiday or a motorized/mechanized military unit, I don't think the system above is practical realistically practical in the environments that we focused on in the paper.
Adam (Full Disclosure: I'm one of the authors)
There is a safe water option, which is simple, economical and effective: http://www.lifesaversystems.com/lifesaver-products/lifesaver-jerrycan
From their home page: 'LIFESAVER® technology filters down to 15 nanometres, that is 0.015microns. We are the world's first and only portable technology that is patented worldwide, to filter down to this level. With the smallest virus known being Polio at 25 nanometers, you are safe in the knowledge that LIFESAVER® filters all bacteria, viruses, cysts and all waterborne pathogens from your water.
The LIFESAVER® jerrycan carries 18.5 litres of water (at one time) and allows users to process up to 20,000 litres of clean sterile drinking water. The LIFESAVER® jerrycan allows the user to stay out for longer as they are no longer dependent on bottled water'.
I watched a TV documentary on this a few years ago and wonder why aid providers do not buy them in bulk.