The Need for Clear Language in Ready Medical Force Requirements
Franklin C. Annis
Unlike the other branches in the Army, the Army Medical Department (AMEDD) hasn’t had clear tasks requirements for officers since the 1990s. It is unknown why AMEDD stopped the practice that was universal to the rest of the Army. This has left the AMEDD in an awkward situation of not being able to clearly define, measure, track, communicate, and estimate the cost of the critical Ready Medical skills that are required on the modern battlefield. To be clear, the “Ready Medical Force” represents the AMEDD personnel fully trained, experienced, and prepared to deploy in their war-time mission. While AMEDD personnel have performed to the highest-level to preserve life on the battlefields of Iraq and Afghanistan, we should continue to improve the quality of our services. There is a need to conduct a critical examination and to clearly define the operational and institutional requirements of each medical specialty in order to meet the demands of expeditionary medicine. A system to track the training and operational experience of our AMEDD specialties could greatly assist in determining readiness, enhancing talent management, informing commanders, and providing needed information to estimate the cost to prepare medical personnel for the expeditionary environment.
The challenges during this examination of what should be the requirements of medical providers is the lack of clear language that captures the intent of the Ready Medical Force initiative. The current language the Army possesses almost exclusively belongs in the institutional (training) domain of leader development. Unlike other branches that necessitate specific training requirements to be considered validated for expeditionary deployments, AMEDD is placing emphasis on operational experience and only defaulting to institutional requirements when providers are unable to acquire specific numbers of operational experiences. This is causing the AMEDD to use institutional language in defining operational experiences. This creates significant problems as “stretching” these institutional terms into the operational domain may create more confusion than it resolves. Instead of using correct doctrinal terms and concepts, AMEDD is essentially redefining these terms and creating a language that will not be understood by those outside our branch. During this process, it may be appropriate to take the time to create and define the terms for the unique way that AMEDD intends to validate its Ready Medical Force.
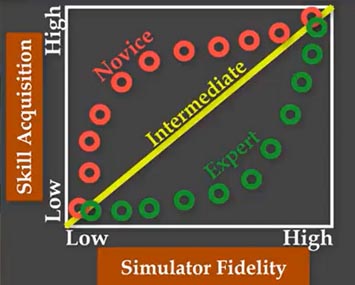
Figure 1 – Skills Acquisition verse Simulator Fidelity. (Aggarwal, Mytton, Derbew, Hanael, Heydenburg, Issenberg, MacAulay, Macini, Morimoto, Soper, Ziv & Reznick, 2010)
The focus on operational experience over institutional training in AMEDD is unique (The nearest comparison might be the flight hour requirements in Aviation). Imagine if we asked an infantry Soldier to demonstrate the task of clearing a stoppage of a M-4 carbine. Would we ever accept the record that he had done so recently in an operational environment as “credit” to fulfill this task? The answer would be no. We would expect this soldier to perform this function as part of some training event to validate this task. However in AMEDD, we are clearly putting the emphasis on operational experiences and only accepting institutional training when required to close the gap. In short, we don’t want providers “trained” for surgery, we want providers “experienced” in surgery. To give a hypothetical example of the emerging requirements, surgeons might be required to “assess, preform, and document, “X” number of long-bone surgeries” as part of their validation process. AMEDD rightfully is placing the emphasis operational experience (i.g. medical interventions preformed on real patients) of its force. If a provider was unable to acquire enough procedures to validate their requirement, they could possibly execute high-fidelity simulation training to make up the difference. Operational experience (“real world” patients) is a superior method to ensure skills acquisition and retention. While simulation can also provide skills acquisition and retention, to attempt to duplicate the same level of acquisition as operational experience requires high-fidelity simulations systems that are highly resource dependent. For more information on the impact of simulator fidelity (realism) on skills acquisition, click here.
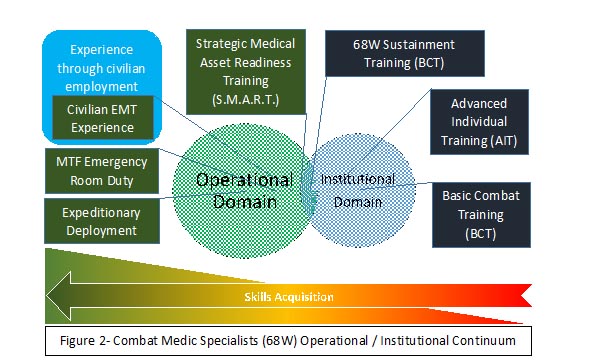
Figure 2 displays the operational/institutional continuum for hypothetical National Guard Combat Medic Specialists. You can see how a Soldier could progress (from left to right) in their skills development through Basic Combat Training (BCT) to a combat deployment. The experiences of BCT, Advanced Individual Training (AIT), and 68W Sustainment fit within the scope of the institutional domain. A language problem occurs once we encounter programs like the Strategic Medical Asset Readiness Training (SMART) program. When I first encountered this program, I was told it is a “training experience without a curriculum.” The lack of a curriculum should be a major indicator that this experience might be in conflicts with the definition the Army uses for “training” courses. The lack of “structure” to these experiences would place them outside the Army definition of training (AR 350-1, 2017, p. 28). The purpose of the SMART program was to allow medical specialists of various Area of Concentrations (AOCs)/Military Occupation Specialties (MOSs) to operate in a civilian medical environment to gain operational experience. In this way, it might be better defined or thought of as an “operational assignment” even if it is only 14 days at a time. While it is highly likely that our AMEDD personnel will be mentored and developed by the more experienced civilian staff in these hospitals, engaging in mentoring isn’t enough to classify this experience as training. I absolutely hate to break a cool acronym such as SMART, but the “T” should be an “O” or maybe “OE” for Operational experience. The lack of clearly defined and applied terms, to include the Army having a lack of a concise definition of “Operational experience,” will continue to cause conflict and misunderstanding as we work towards a solution. Perhaps a program name like Operational Ready Medical Development (ORMD), spoken as “OR””MD” to allude to a doctor in an operating room, might better fit the bill.
As we move forward with the Ready Medical Force initiative, we need to be careful and clear in our communications. This might mean recognizing when the intent of the current initiative exceed the definitions that currently exist within doctrine. This might require AMEDD to invest the time to create new terms and language to ensure this initiative can reach its end goal and be understood by non-AMEDD commanders and personnel. We want to create an environment where non-AMEDD commanders will not be confused by the formatting of the Ready Medical requirements of their medics. Recognizing the need for clear language in the opening phases of this initiative could save us a lot of heartache in the future.
References
Aggarwal R, Mytton O.T., Derbrew, M., Hananel, D., Heydenburg, M., Issenberg, B., MacAulay, C., Mancini, M. E., Morimoto, T., Soper, N., Ziv, A., & Reznick, R. (2010) Training and simulation for patient safety, BMJ Quality & Safety, 19:i34-i43. http://qualitysafety.bmj.com/content/19/Suppl_2/i34
Headquarters, Department of the Army (2017), Army Regulation (AR) 350-1, (Government Printing Office: Washington, DC).
About the Author(s)
Comments
The difficulties during this…
The difficulties during this assessment of what ought to be the necessities of clinical suppliers is the absence of clear language that catches the goal of the Ready Medical Force drive click here for more info Top essay writing mission revolves around the students, all else being equal paying little attention to where they live or what they study. We try to make their life more simple by giving them fast and proper help.