U.S. Naval War College - Humanitarian Response Program
Pandemic Response: Select Research & Game Findings - April 1, 2020
Introduction
This document is a summary of 16 key research and game findings focused specifically on the characteristics of civil-military response to a pandemic scenario. The numbered bullets below correspond to more detailed explanations of findings presented later in the document. While these findings are in no way definitive or complete, they are a sampling of relevant guidance based on research, gaming and expert opinion. It is our hope that these 16 findings will contribute to improving civilian and military effectiveness in humanitarian assistance and disaster response operations.
Note on Urban Outbreak 2019
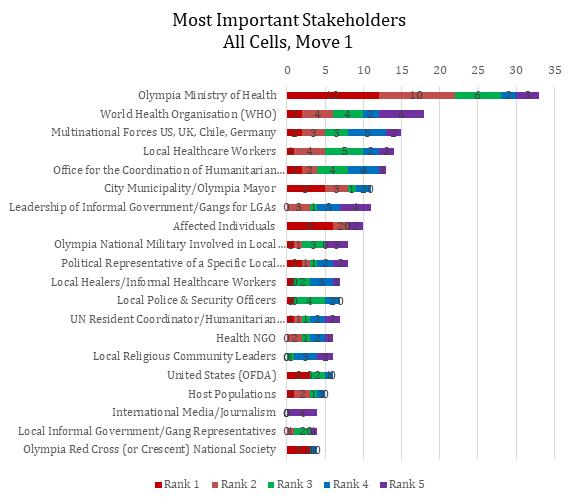
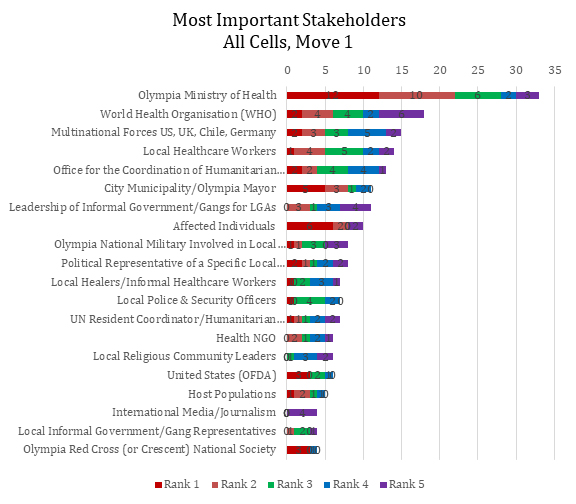
The document references “Urban Outbreak 2019,” which was an analytic war game designed, delivered and analyzed by NWC’s Humanitarian Response Program in collaboration with Uniformed Services University of the Health Sciences (USUHS) - National Center for Disaster Medicine and Public Health (NCDMPH) and Johns Hopkins University’s Applied Physics Lab. In September 2019, Urban Outbreak brought together 50 experts from five different sectors who averaged 10 years of humanitarian response experience. Over two days they gamed an infectious disease outbreak response in a notional but realistic city with a population of 21 million people. As part of the game, players individually voted for up to five essential organizations to which they needed access in order to complete the activities they deemed essential for success in the response. Histograms of those votes are offered in appendix I & II. The scenario-based aspects of the game that focused specifically on the unique characteristics of urban response in a widespread outbreak are also listed in appendix III.
Select Research & Game Findings[i]
Early actions and planning across all sectors are exponentially more important than reactive measures once the disease is widespread.
There will be intense and overwhelming demands for access to a few key health related organizations that are viewed as authorities in the early stages of a response. As the response moves forward, the number of stakeholders who are in high demand will increase and diversify.
While a response will often focus on serving the infected, any response must also focus on all the ways to lower the R “naught” or R0 (the average number of people infected by each new person infected). Regularly identifying high-risk practices that raise the R0 and replacing them with suitable alternatives for a population is an exceptionally difficult and absolutely essential factor for success.
Forced mass quarantine or other top down approaches to an outbreak that securitize the response with law enforcement and/or military enforcement may not be successful and could increase the spread of the disease.
Questioning the data central to planning and operations in an outbreak is an essential reflex that needs to be developed and sustained throughout an organization.
Currently, mortality is a better indicator of the scale of the COVID-19 outbreak than lab confirmed case counts. These facts on the ground are inherently lagging a couple weeks behind infections, but without real time and widespread testing of infections, mortality offers tangible and reliable data. Mortality “doubling time” is the most important and widely accessible metric for winning the race against COVID-19 in the absence of extensive testing.
Establish local media relationships early for risk communication as outbreak intensifies. In order to effectively combat misinformation and rumors, risk communication should be hyper-local, establish a track record for truth early, and directly involve known community members with a stated focus of honesty over polished language or production value.
Responders may be overconfident if they are not directly connected to the field. Frontline healthcare workers and first responders are often a good source of realistic assessments.
Personal and professional risk tolerance for humanitarian response activities is generally much higher for non-governmental organizations and medical first responders than it is for the military and U.S. government employees.
Even in the planning phase, the military and government may (consciously or unconsciously) exhibit avoidance behaviors to limit the scope of their involvement with affected and/or infected populations in the field.
A highly unusual mission and/or unprecedented response conditions such as pandemic response will meet with significant resistance, even among experienced professionals. This can directly inhibit effective planning and adaptation.
Private sector organizations are an absolutely essential and uniquely nimble component of any large-scale response. They must be integrated into planning throughout all phases of a response.
The U.S. government may need to clarify the difference between an “outbreak response” and a “humanitarian disaster” though these activities are not mutually exclusive.
Health care, drugs or other treatments should be provided through whatever means people are accustomed to within their local communities.
Social norms will change during a period of crisis; this demands careful observation and adaptation.
Responding organizations may not be aware that some response activities will not scale to meet the demands of an outbreak as they might for other disasters.
Expanded Findings
1. Early actions and planning are exponentially more important than reactive measures once the disease is widespread. Any containment strategy requires testing and tracing. This is not possible once a large enough population is infected. In the same way, altering business, social or cultural practices is significantly less effective when a society is facing a wide range of new challenges, especially severe economic and social pressures. Clarity, speed and repetition are essential for changes within a population and are most effectively achieved before other factors start making decisions for them. Generally, any action taken after a virus is widespread will be less effective due to the virus’ impact on society. The larger and more complicated the action, the more the impact of the disease will be felt in its execution.
2. There will be intense and overwhelming demand for access to a few key health related organizations that are viewed as authorities in the early stages of a response. As the response moves forward, the number of stakeholders who are in high demand will increase and diversify. Urban Outbreak Example: After a shared briefing, 66% of the players voted that the Ministry of Health was the most essential stakeholder to which they needed access to complete their response activities during the initial outbreak. When players voted again after the briefing at the apex of the outbreak, their priorities for access had diversified by approximately 20% across a wider range of stakeholders. Players also voted to add approximately 30% more stakeholders as essential to their response activities. See histograms below.
3. While a response will often focus on serving the infected, any response must also focus on all the ways we can lower the R0. Pandemics are a function of human behavior mixed with a pathogen that has a specific R “naught” or R0. The R0 represents a simple average of how many people each infected person will infect. So R1.5 would mean everyone who gets the disease gives it to one and a half other people. The important thing to remember is the R3 means an exponential growth curve for the disease but it is not a fixed number. The R0 is a product of all the behaviors and environmental factors that result in those three new infections. So if society can change how they behave or alter the environment to lower that R3 to an R1 (or lower) while treating the infected, the disease will not be able to replicate enough to survive. In some cases this could be as simple as hand washing or social distancing, in other cases like Ebola it may clash with longstanding cultural practices like body preparation and burial by hand. Regularly identifying these high-risk practices that raise the R0 and replacing them with suitable alternatives for a population is an exceptionally difficult and absolutely essential factor for success.
4. Forced mass quarantine or any other top down approach to an outbreak securitizes the response. This may not be successful and could increase the spread of the disease. Sick people actively seeking care, testing and public health messages concerning self-isolation and quarantine of contacts are the ways to end outbreaks. Forced mass quarantines are a direct barrier to those activities. One cannot slow the spread of disease if people hide infections out of fear or stigma. When authorities attempt to enforce a mass quarantine on a large population they will not be 100% effective. By stigmatizing the infection and symptoms they will teach others to hide their symptoms and drive key populations underground. This results in less sharing of information with authorities and medical providers, and the most desperate and the highest risk populations will seek to break quarantine.
5. Questioning the data central to planning and operations in an outbreak is an essential reflex that needs to be developed and sustained throughout an organization. Data collection, analysis and dissemination in a disaster response are by their very nature contentious political activities. Responders require data to execute their responses but rarely do the data collection and analysis themselves. This can lead to a significant weakness related to outbreaks as responders can base too many of their major decisions on external findings that may be dated, inaccurate, or misleading. Example from Urban Outbreak: There was no questioning or rejection of the epidemiological reports given to the players even though the infection curve did not follow the normal trajectory for this type of outbreak. This was especially apparent in the final round when there was no clear indicator of why the reported number of infections had fallen dramatically and yet many of the players embraced the idea that it was due to a successful response. This was concerning because designers anticipated questions about data collection and reliability by such a wide array of seasoned experts but not blind acceptance of such abnormal reports.
6. Currently, mortality is a better indicator of the scale of the COVID-19 outbreak than lab confirmed case counts. These facts on the ground are inherently lagging a couple weeks behind infections, but without real time and widespread testing of infections, mortality offers tangible and reliable data. While there is a great deal of data emerging about infection rates in the United States it is inherently behind the infection curve, incomplete and unreliable. For this reason, mortality is a better indicator of the scale of the COVID-19 outbreak than lab confirmed case counts. While even this number has room for error and each death for COVID-19 is estimated to take 13-17 days - causing a long lag between interventions and results. It is more manageable data and allows rough calculations for decision-making. For example, instead of attempting to measure the number of infected, experts have offered that lengthening the number of days it takes mortality to double or “doubling time” is the most important and widely accessible metric for winning the race against COVID-19 in the absence of extensive testing. The further from three days the doubling time gets, the further a population is from the runaway period of the pandemic.
7. Establish local media relationships early for risk communication as outbreak intensifies. Urban Outbreak Example: Upon reaching the apex of the outbreak in round two NGOs and some U.S. Government (USG) independently identified a shift from national to local media outlets and dissemination, focusing on TV, radio, and billboards for “carpet bombing” public health messaging (as opposed to web, national or international) in order to build local trust, relevance, and community response rate. It will also increase a responder’s control over speed of delivery and accuracy.
When focused on protecting public health, authenticity, truth and actionable information are the currency of successful risk communications. This is directly at odds with crisis communication, which is intended to shape messages to defend, protect or promote a particular brand or interest. In a sustained crisis the public will become increasingly dismissive of messages that don’t reflect the immediacy or intensity of their experience or sentiments. In order to effectively combat misinformation and rumors, risk communication should be hyper-local, establish a track record for truth early, and directly involve known community members with a stated focus of honesty over polished language or production value. To maintain legitimacy in risk communication, inconsistencies in messages, response failures and/or public expressions of intense anger or grief should not be omitted or censored. Instead, they should be voiced, explained and offered as legitimate and understandable aspects of a community wide crisis.
8. Responders may be overconfident if they are not directly connected to the field. Frontline healthcare workers are often a good source of more realistic assessments. Example from Urban Outbreak: Players in round one (early onset) and round two (outbreak apex) were asked to rank their confidence in their ability to complete their priority activities if they had full access to those essential stakeholders they selected. In their post move survey they were asked to rate their assessment of the impact their priority activities would have on the overall response. There was no significant change in confidence by any group except for Bravo Cell even though the outbreak grew exponentially. Participants in Bravo Cell – (NGO players), were statistically less confident in their ability to achieve their first priority activity between move one and move two. This confidence measure was from the only group focused on directly serving the affected population through medical care and other local programing. They were inherently more connected to the reality of directly running diverse patient-facing medical and public health programs. They are also highly aware of the personal risks they have to manage or mitigate as the programmatic leads in the field.
9. Personal and professional risk tolerance for humanitarian response activities is generally much higher for non-governmental organizations and medical first responders than it is for the military and US government employees. Urban Outbreak Example: Humanitarian organizations were significantly more engaged in the problem set on the ground than their military or government counterparts. While fully aware of security and logistical challenges in front of them, humanitarians and healthcare workers think in terms of baseline conditions for access, program rollout and sustainment first and consider complicating factors second. Military and government generally focus on authorities, mission parameters, personal security and other similar issues for an exceedingly longer time before even considering the functional factors involved in the effective execution of a mission or program. As the military and government engage in that early planning phase, they identify a great deal more reasons why they cannot do something rather than how they can. It is the opposite for humanitarians and healthcare workers because their work is predicated on the idea of responding unless there is an absolutely unacceptable risk. This can lead to cultural clash when collaborating. For example in Urban Outbreak, humanitarians became frustrated with discussion points offered by the military and USAID explaining:
“Health care workers don’t need to waste time discussing coordination or mission drift – coordination is an activity you do and our mission is the population in front of us.”
10. Even in the planning phase, the military and government may (consciously or unconsciously) exhibit avoidance behaviors to limit the scope of their involvement with affected and/or infected populations in the field. Urban Outbreak Example: This was highly apparent across a wide range of military and USG (e.g. CDC, HHS, USAID) players. Avoidance behaviors were most often exhibited as redirection of discussions and moves related to serving affected populations towards nebulous high-level policy issues, minutia of command structures, and coordination imperatives. When pushed towards planning direct response activities, these players often used coordination with other “expert” organizations to passively externalize any personal or organizational risk of direct engagement with the population. The fact that these players knew the infection in the game was curable (with moderate immunity) with just two doses of antibiotics but actively avoided discussing distribution, or prophylactic force protection, lends credence to this interpretation. Humanitarians almost exclusively voted for affected/infected populations, as their most essential stakeholder to access, while other players did not vote for them at all. This shows a significant gap in the response community, as direct assistance to the infected will be a primary and overwhelming task in a pandemic.
11. A highly unusual mission and/or unprecedented response conditions will meet with significant resistance, even among experienced professionals. This can directly inhibit effective planning and adaptation. In the design and execution of the Urban Outbreak, experts at all levels sometimes vehemently rejected those game elements that they felt were too foreign to their experience. The original pathogen proposed for the game had an R0 closer to the COVID-19 virus, exhibited itself with cold and flu like symptoms, and required long-term intensive medical care for a small portion of the population. This proposal was rejected for a variant of a known and curable bacterial pathogen. The learning opportunity lost by failing to use the original pathogen proposed is now obvious.
Urban Outbreak Example: During gameplay players would often exhibit physical discomfort and become argumentative concerning those aspects of the scenario that did not conform to their previous experience. This occurred even when other experts in the room would vouch for the scenario’s veracity and relevance. The concern is that these reactions generally led resistant players to ignore or overlook good resources and guidance in their problem solving. If left unchecked it can often lead to a groupthink sentiment of “different is dangerous,” with an obvious impact on effectiveness. This was exhibited in the game as key groups failed to engage in new and different aspects of the scenario (e.g. unique urban environment, mass antibiotic distribution, cooperation with local gangs) and instead retreated to exploration of known quantities, (e.g. C2 structures or information gathering activities).
12. Private sector organizations are an absolutely essential and uniquely nimble component of any large-scale response. Urban Outbreak Example: A lead for a private sector logistics company offered some of the most tangible and innovative approaches to the problem set. The solution from his standpoint was to maintain business continuity (even while taking losses) by ensuring everyone on his payroll and their families had early access to antibiotics. He was confident his business would already have devoted members of local gangs and their families on the payroll as employees and so his early interest in their health and safety would open up the supply lines he would be able to use throughout the response. However, he had no interest in using overland shipping options due to security concerns and poor road infrastructure and instead sought to ferry all goods on waterways by employing a public private partnership with the local transit authority. With this strategy he was able to divide up most of the population centers and reach them without military support, air assets or many changes to his existing business model.
13. The U.S. Government may need to clarify the difference between an “outbreak response” and a “humanitarian disaster” though these activities are not mutually exclusive. Urban Outbreak Example: There was broad agreement among USG players that round one was an “outbreak response” which required more of a testing, contact tracing and health advisory role while round two was a “humanitarian disaster” requiring a different approach. There was still limited discussion of actually engaging the infected population. Priorities became personal security, disease surveillance, restricting movement by decentralizing resources, and looking for public health response mechanisms outside of health systems (e.g. sanitation efforts).
14. Health care, drugs or other treatments should be provided through whatever means people are accustomed within their communities. Urban Outbreak Example: In order to implement programs that are quickly accepted and effective with minimal disruption in dense urban areas, the international response needed to provide drugs, testing and aid through pre-established pharmacies, community organizations, religious leaders or practitioners without caveats.
15. Social norms will change during a period of crisis. Some changes may be characterized as normal coping mechanisms, but flagrant criminal activity must be actively pursued to reinforce social norms. The black market will inevitably become a critical factor as market pressures increase risk, reward and opportunity. Crime will also increase given the same factors, but including economic desperation and an opportunistic “testing” of authorities’ control. Drug use, alcoholism and domestic abuse will noticeably increase. Every action by authorities may have magnified implications for individuals, families and communities.
16. Responding organizations may not be aware that some response activities will not scale in the way that they normally would. Urban Outbreak Example: Red Cross Movements continuously took the role of respectful and culturally appropriate mortuary affairs but they were never asked how they would manage disposal of 90,000 bodies in three months nor did they ever explain that capability. Under normal circumstances this wouldn’t be an issue, but under extreme circumstances even highly effective and established organizations should reconsider their capacity over their capabilities.
Contributing Authors
Benjamin Davies
Kaitlin Rainwater Lovett
Brittany Card
David Polatty
Analytic Contributors
Alexandra Whiting
David Weinstein
A Note on Results Interpretation
The following histograms from Urban Outbreak 2019 show vote type and frequency from fifty players but they also show vote priority. Players were instructed that their vote order meant higher or lower levels of access to the external stakeholders they selected. A player’s first vote was their highest priority stakeholder descending to their fifth vote. Players could choose from a list of 100 pre-identified organizations or add organizations. The first histogram shows the vote following the initial outbreak and activation of a response. The second histogram shows the vote at the height of the outbreak.
Appendix I
Appendix II
Appendix III
Urban Challenges and Areas of Inquiry in Urban Outbreak 2019 Scenario
Round One: Outbreak
- Concept of employing informal public health providers in the response
- Concept of informal governance/security for access or mobility for vulnerable populations in key dense urban areas
- Establishing role of private security
- Determining differential access to resources based on social strata and location
- Assessment data from rural mountainous region
- Self-interested government officials and private sector actors
- Prostitution as a vector
- False information/suspicion concerning the outbreak and response
Round Two: Cascading Failures
- Loss of power, utilities, dockworkers, security, etc.
- Failure of existing medical system
- All other medical services severely affected
- Logistical capacity stretched for outbreak response purposes at the expense of all else
- Hoarding, theft, and black market becomes extremely lucrative
- Increased international military role
- Challenges for responder security and ROE for military
- Ambiguous role of the national government
- Role of informal transit for response
- Flight of populations
- Quarantine/roadblocks
- Mortuary affairs
- PPE and medical demand
Round Three: Cleanup Wish List
- Pre-transition change in priorities
- Engineering, heavy lift or logistics from international military before transition begins/departure
- Reviving broken livelihoods
- Mortuary affairs
- Refuse in urban areas
- Security - rise of gangs and religious groups
- Badly damaged infrastructure
- Hobbled workforce
- Extreme needs associated with fractured health system (public health emergencies associated with those failures)
End Note
[i] The views presented by the faculty and contributors do not reflect official positions of the Naval War College, DON or DOD.
About the Author(s)

Comments
If you want a future where…
If you want a future where students are just given facts, information and they rote it, then online education is fine. But it's not real education. I suggest reading the article on how to cheat Turnitin, it's useful for every student when they study online.
We are committed to…
We are committed to providing our clients with exceptional solutions while offering web design and development services, graphic design services, organic SEO services, social media services, digital marketing services, server management services and Graphic Design Company in USA.
Amazing that colleges reveal…
Amazing that colleges reveal such initiative in response to the pandemic that changed our lives. I am a busy student and when it gets too difficult to handle the assignments, I go to useful source to read the review and choose the professionals who will make my study much easier.