Trained But Undeveloped: Rethinking Combat Medic Sustainment
Franklin C. Annis
In the fall of 2009, I found myself as a Platoon Leader of 26 Combat Medics (68W) deployed to Iraq. To my horror, I discovered the vast majority of my medics had never treated a “real” patient. The majority of them only had experiences provided in Military Occupational Specialty (MOS) and MOS Sustainment Training. These experiences were limited to training and education during their Advanced Individual Training (AIT) with no more than a 3-day experience being closely monitored while working within the Brooke Army Medical Center. I faced the hard reality of assigning significant numbers of “untested” medics to combat logistics patrol missions. Being the only medical provider within the convoy, these medics would be truly tested “under fire” in the event of a serious injury.
The concern for the lack of operational experience of my combat medics came from my own personal experience within emergency medicine. I graduated from the Creighton University Paramedic Program and spent countless hours on ambulances, in Omaha and the surrounding area, gaining valuable experience in treating “real-world” patients. In these experiences, I learned how to react to the smell of bodily fluids. I learned the emotional terror of treating an unresponsive infant. I watched patients die and dealt with the emotional reactions of their families. All these experiences are near impossible to reproduce to full-significance even in the best simulation and training scenarios. Finally, I watched some of my peers find they were unsuited for the mental strain of emergency medical services. While encountering a mass-casualty event involving a school bus, one of my peers became overwhelmed by the experience and became non-functional as a medic. Luckily, this was in an environment where there were other emergency responders on scene. What would happen if my “untested” medics froze on contact? Are we really prepared to send inexperienced medics into harm’s way when they are responsible for the lives of American service members?
The Army has a Leader Development Model that records the need for Operational (Experience), Institutional (Training & Education), and Self-Development Domains to optimize Army leaders (Figure 1). While this model was originally intended to focus on Army leadership development, the three domains could be applied to any developmental needs of Soldiers. The Institutional domain is critical for learning the theoretical skills, behaviors, and knowledge of the profession. It is the Operational domain that allows individuals to tests these skills, behaviors and knowledge in new and unfamiliar situations. Finally, Self-Development allows individuals to optimize their performance and drive innovation.
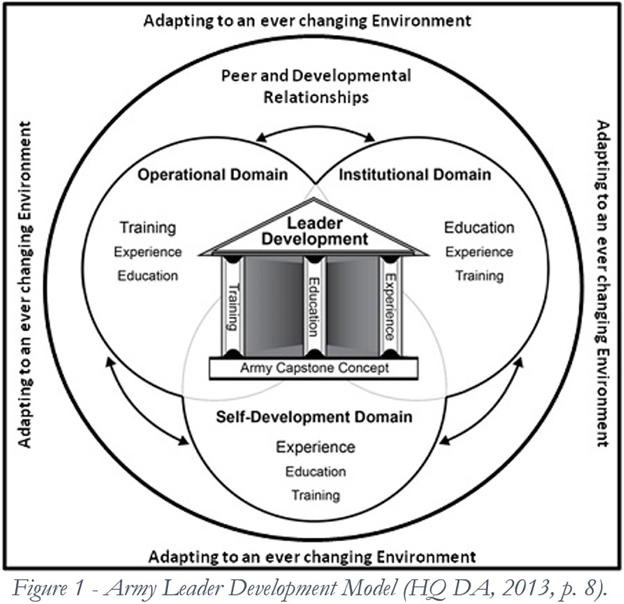
Currently the development of Combat Medics is too heavily focused within the Institutional domain and needs the immediate introduction of the Operational domain to improve the abilities of Army medics. Offering supporting materials for Self-Development could further optimize the performance of Combat Medics on the modern battlefield.
Current Training Requirements
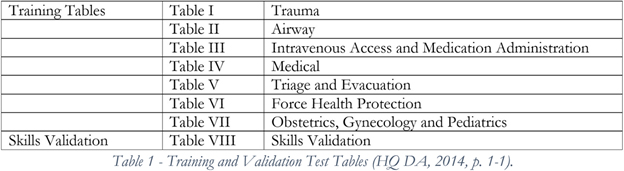
The volume of Combat Medics trained at Fort Sam Houston, Texas is likely prohibitive in providing more patient contact during AIT. So, we will look towards sustainment training requirements as an area to possibly support more engagement in the Operational Domain with live patient encounters. The current MOS sustainment training requires: 1) Biennial recertification as an Emergency Medical Technician-Basic with the National Registry of Emergency Medical Technicians (NREMT). 2) Basic Life Support Healthcare Provider certification (American Heart Association or Military Training Network). 3) Minimum of a biennial skills validation through completion of Tables I – VIII of Training Circular (TC) 8-800 (Table 1). 4) A minimum completion of 72 hours of Continuing Education (CE). While the training support package (TSP) within TC 8-800 intends Combat Medics to complete Tables I-VIII on an annual basis to fulfill the CE requirements, many units and Soldiers find it difficult to complete this model and have to default to some form of alternate CE acquisition.
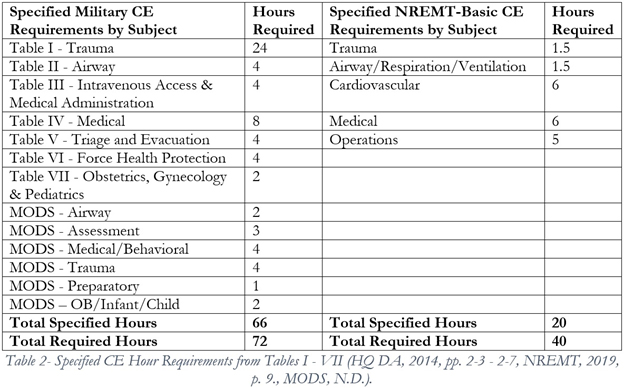
It is to be noted that the 72 hour requirement for CE exceeds the recertification requirements of the NREMT by 32 hours (Table 2). By providing more options to complete the 24 hours of CE above the skill validation requirements of TC 8-800 (Tables I-VIII) may be an effective means of introducing more Operational experience (civilian ambulance ride along, work in emergency rooms, etc) in the development of our Combat Medics. Allowing for an Operational experience in lieu of training would require us to assume risk in that all Operational experiences are not identical. However, it would be incredibly short-sighted for the Army to prefer an inferior training protocol that is more easily credentialed because of its uniformity instead of embracing a superior development environment that displays a greater degree of variance.
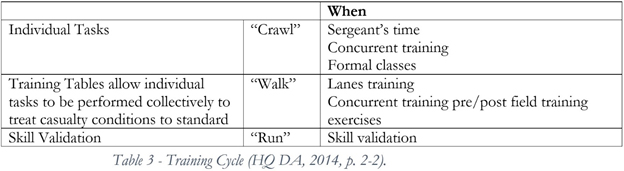
Providing an Operational experience in lieu of the 24 hours of CE would advance the established training cycle for Combat Medics (Table 3). The “Crawl, Walk, Run” training modality has served the U.S. Army well. Expanding on this analogy, providing an Operational experience (such as an ambulance ride along) would be the equivalent to “sprinting.”
I find the objection to allowing an Operational experience due to the inconsistency of experiences as invalid. Civilian paramedic programs across the country require Operational experiences as a foundational component within their training/education programs. Clearly, these institutions have developed protocols to establish relationships and ride along programs that ensure high-levels of patient contact. The Strategic Medical Asset Readiness Training (SMART) line of effort is a perfect example of the Army copying these types of programs working with major civilian trauma centers to ensure quality Operational experiences. The additional 24 CE requirement holds little educational value when completed through the typical online courses (currently provided by Relias). A “real-life” patient would provide infinitely more skills obtainment and can develop other critical traits (like confidence) that cannot be taught via distance education. In limited Operational experiences, like SMART, Combat Medics can gain confidence, develop situationally aware skills, test and build their psychological resilience, engage in creative thinking to adapt the emergency scene, and work on communication and teamwork skills in a mentored environment.
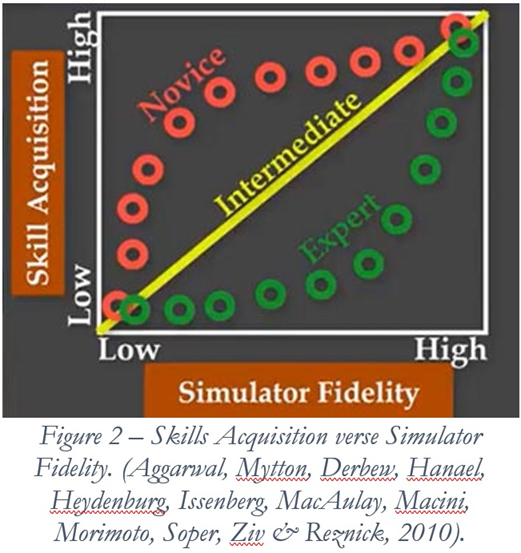
Even if we had the resources to put all Combat Medics through high-fidelity simulations for this additional 24-hour CE requirement, an Operational experience would still be a superior learning modality. I will admit that “live” patients in the civilian environment would not replicate the “combat” elements of a deployed environment. However, the skills validation in TC 8-800 would re-enforce the “tactical” skills required for combat. It is to be noted that even in our finest simulations, we cannot accurately reproduce the actions and reactions of “live” patients. Simulations are simply not “real” enough to create the same level of skills acquisition as preforming the action on live patients. At the end of the day, the rubber doll is just an inanimate object that will come back to “life” for the next training scenario. If used, the “Standardized patient” (Actor) wasn’t in a life and death situation. The smell and feel of simulated blood will never exactly duplicate “real life.” Even the best training scenarios will not duplicate the “reality” of life-threatening emergencies and the psychological reactions of the Combat Medic that realizes there is no “reset button.” However, civilian trauma patients can be.
Introducing Operational Experiences
Strategic Medical Asset Readiness Training (SMART) line of effort, run by the Office of the Surgeon General, provides a good example of how operational experiences could be integrated into the Combat Medic sustainment training curriculum. While I do have issue with the term “training” in the SMART name, SMART provides an exceptional opportunity for medical personnel to work in their specialty within a civilian hospital system for a 13-day rotation. While this line of effort was originally designed to support the skill retention of low-density medical specialists, Combat Medics have been taking advantage of working within the Emergency Rooms and, in some cases, the ambulances of the supporting major civilian medical centers. This experience could be viewed as a mini-deployment experience providing much needed Operational experience.
This roughly two-week experience can build multiple skills that cannot be built within the current training protocols. Combat Medics participating in this line of effort have an opportunity to work on their bedside manner and build psychological resilience by being introduced to controlled, yet stressful, live patient encounters. SMART offers a means of engaging in stress inoculation while building a Medic’s confidence.
While SMART is still in its infancy and could not currently support a training rotation for all the Combat Medics within the U.S. Army, the Army should continue to invest heavily into this type of line of effort and enjoy the benefits of more experienced medics. The Army EMS Program Management Office should immediately consider shifting the Combat Medic Sustainment Program from one that focuses solely on the Institutional domain to one that includes the Operational domain and encourages engagement with the domain of Self-Development. This would bring the Combat Medic Sustainment Program more in line with the newly created Individual Critical Task Lists (ICTLs) The ICTLs were recently designed for the various Medical Officer specialties which included requirements for both training and experience. In the end, we should want not just trained, but experienced medical providers. Allowing the additional 24 hours of CE to be completed via an Operational experience like SMART would ultimately shift the focus on Combat Medic sustainment from one of training, to one of development.
Self-Development
Encouraging Self-Development among Combat Medics is a topic large enough to justify several books. I will briefly touch on it here as we should be encouraging Combat Medics to learn beyond the minimum requirements of their specialty. One way the Army could encourage Self-Development is to supply Combat Medics with access to additional high-quality instructional materials about emergency medicine. While it has been a number of years since the use of CentreLearn for an online Continuing Education platform, I remember this vender providing countless interesting topics for online instruction. One year I took well over 100 hours of additional training, including topics such a snake bites and snowmobile accidents. While I cannot guarantee that Soldiers would ever need the information provided in these more unique courses, taking these courses will cause Combat Medics to think more deeply about their specialty. Having fun and entertaining material to expand Combat Medics’ capabilities would greatly increase their ability to adapt to the complex and ever-changing realities of the modern battlefield.
Reserve Components
Shifting to a more holistic approach to Combat Medic Sustainment could have significant advantages to the Reserve Components. Members of the Army National Guard and Army Reserves are finding the promise of “one weekend a month, two week a year” to largely be a lie. These Soldiers face the challenges of initial training, various courses for the Non-Commission Officer Education System, Combat Medic Sustainment Training, and collective unit training during Annual Training. Additional activations for deployment and State Active Duty strain the abilities for these Soldiers to have positive relationships with their employers and civilian academic programs (college/universities). Many Army National Guard states require their Combat Medics to attend an additional training period to complete the Combat Medic Sustainment Training. With a commander’s challenges to balance the need of individual verses collective training, lines of efforts like SMART that do not currently provide CE credits for sustainment requirements may be abandoned for far less effective educational modalities. Allowing Reserve Component Combat Medics to receive sustainment “credit” for Operational experiences, like SMART, could have a significant number of advantages. This approach would ensure that all Combat Medics were experienced in emergency medicine. This type of high-tempo experience could drive recruitment and retention among the Reserve Component by allowing Combat Medics to experience the excitement and rewards of working within the field of civilian emergency medicine. Commanders are likely to embrace these types of Operational experiences as they would become part of the sustainment requirements instead of an additional optional experience. It could also assist Soldiers in finding civilian employment within these civilian medical systems.
Shifting from an Institutional Domain to a Development Focus
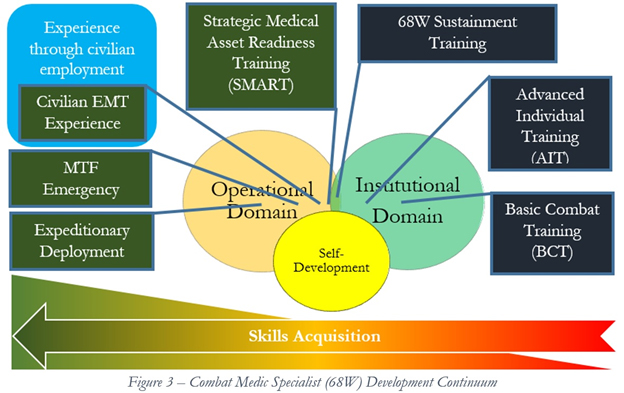
The U.S. Army faces many challenges in preparing Combat Medics for the modern battlefield. The challenges of a near-peer conflict will likely demand more from our Combat Medics than what was experienced in the Long War. To better prepare for the future battlefield, we should consider shifting the focus of our Combat Medic Sustainment Program from one that is purely institutionally focused to one that stresses overall development. One method to adapting a developmental approach would allow for Operational experiences, like the SMART, as credit towards Combat Medic Sustainment requirements. This approach has many advantages including the building of many “soft skills” not developed within a training environment and providing experiences with much greater skills acquisition in lieu of distance education. By understanding the great value in Operational experiences and viewing developmental experience on a continuum (See Figure 3), the Army could start prioritizing and benefiting from greater skills acquisition among their medics.
Conclusion
The Army would greatly benefit by shifting the concept of Combat Medic Sustainment Training to Combat Medic Development. By supporting all three developmental domains (Operational, Institutional, & Self-Development) within Combat Medic Sustainment, the Army could take advantage of greater educational opportunities. If included, lines of efforts like SMART would greatly enhance the confidence and psychological resilience of Combat Medics through Operational experiences within civilian emergency medicine environments. As the U.S. Army continues to adapt for the challenge of a near-peer conflict, it is clear that we will need not only trained but experienced medical providers on the battlefield. Providing Operational experience through lines of efforts like SMART and providing supporting material for Self-Development, the Army could improve its current training protocols to better optimize Combat Medics for the modern battlefield. If nothing else, utilizing this approach would prevent “untested” medics arriving on the battlefield and facing the challenge of treating their first “real” patient where there is no margin for error.
References
Aggarwal. R., Mytton, O.T., Derbrew, M., Hananel, D., Heydenburg, M., Issenberg, B., MacAulay, C., Mancini, M. E., Morimoto, T., Soper, N., Ziv, A., & Reznick, R. (2010). Training and simulation for patient safety, BMJ Quality & Safety, 19:i34-i43. http://qualitysafety.bmj.com/content/19/Suppl_2/i34
Annis, F.C. (2019). The need for clear language in Ready Medical Force requirements. Small Wars Journal. https://smallwarsjournal.com/jrnl/art/need-clear-language-ready-medical-force-requirements
Britzky, H. & P. Szolda. (20 September 2019). Leaked Army document reveals the whole ‘one weekend a month’ reserve thing is kinda b*llshit. https://taskandpurpose.com/army-reserve-weekend-readiness
Headquarters, Department of the Army (HQ DA). (2013). Department of the Army Pamphlet (DA PAM) 350-58, Army leader development program. Washington, DC: Government Printing Office.
Headquarters, Department of the Army (HQ DA). (2014). Training Circular (TC) 8-800, Medical education and demonstration of individual competence. Fort Sam Houston, TX: Government Printing Office.
Medical Operational Data System (MODS), (N.D.). https://logistics.mods.army.mil/EMS
National Registry of Emergency Medical Technicians (NREMT). (2019). Recertification guide. Columbus, OH: National Registry of Emergency Medical Technicians, Inc. https://content.nremt.org/static/documents/Recertification%20Guide.pdf
US Army EMS Program Management Division (Army EMS). (2017). Standard operating procedure. Fort Sam Houston, TX: Government Printing Office.
About the Author(s)
Comments
We are committed to…
We are committed to providing our clients with exceptional solutions while offering web design and development services, graphic design services, organic SEO services, social media services, digital marketing services, server management services and Graphic Design Company in USA.