“TRAuma Care In a Rucksack” (TRACIR), a Disruptive Technology Concept
Jan Berkow and Ron Poropatich

Introduction
Trauma care in future military environments will require medical technological innovations for an integrated force with the attributes and capabilities to mitigate risks and maximize clinical effectiveness in an Anti-Access, Area Denial (A2/AD) insurgency scenario. [1] According to the U.S. Army Roadmap for Unmanned Aerial Systems 2010-2035 [2], the aviation force mix will shift to mostly unmanned and optionally piloted vehicles. This necessitates accompanying autonomous and semi-autonomous Tactical Combat Casualty Care (TCCC) capabilities to support future UAS missions.
From the Medical Command Operational Order document, the Secretary of the Army and Chief of Staff Army (SECARMY)/(CSA) have initiated Force 2025 and Beyond (F2025B) - a holistic modernization strategy to develop and deliver Landpower concepts and capabilities to the Joint Force and integration into Doctrine, Organizations, Training, Materiel, Leadership, Personnel, Facilities, and Policy (DOTMLPF-P). [3] This strategy will field interim solutions to complete Army 2020, develop and field required capabilities for Force 2025, and set the conditions for forces in the far term horizon of 2040. The Chief of Staff of the Army envisions a future Army that is expeditionary, lethal, responsive, engaged and that is capable of shaping the operational environment. This vision will shape the future force requirements to include combat casualty care and medical evacuation, utilizing both autonomous and semi-autonomous systems.
To address the autonomous requirement, it is posited that the practice of TCCC must undergo disruptive changes that enable the development of an “intelligent” TCCC platform. Applying concepts similar to those employed in robotics, an intelligent system is one that “has the ability to recognize objects and events and to represent knowledge in a world model”. [4] Further, “it is the integration of knowledge and feedback into a sensory-interactive, goal-directed control system that can make plans and generate effective, purposeful action directed towards achieving them”. [4]
It is further posited that the starting point to construct an intelligent TCCC platform demands the capture of quantifiable biomarkers that enable recognition of a trauma event and are supportive of trauma model development. This requires a paradigm shift in the practice of operational medicine from an “art” that employs subjective measures to assess and treat, to a “science” based on employing objective quantifiable measures. This will in turn, provide a fundamental change to the form of medical data that is captured, enable a more accurate depiction of poly-trauma model complexities, and an accounting of those tactical and operational practices to assess goal-directed effectiveness based on data derived actionable knowledge.
This change will also address several military operational needs identified during the period of 2001-2013 that include more accurate data collection from point of injury to a Role 3 facility as well as dissemination of patient status to enable improved telemedicine support and casualty care hand-over through the echelons of care. [5] This form of “operationalized “ medical data will also enable the trauma registry to serve as a tactical knowledge repository to which analytics can be more effectively applied, offering greater opportunity for continuous improvement of TCCC protocols.
Autonomous care also requires the pursuit of challenging critical care interventional system advances that can support closed-loop cardio-pulmonary resuscitation and robotic-driven imaging technologies to enable more precise patient assessments or guide critical care interventions during ground or air transport. The TCCC platform must also undergo a significant change in form factor (cube and weight) that is conducive to a transportable rapid deployment scenario such that it can fit into a Rucksack. This will require miniaturization of these advanced medical tools that can be quickly set up by one person near the point of injury. System portability also addresses the versatility requirement needed to support the use of any casualty for any “vehicle of opportunity” designated for casualty evacuation. These disruptive technology advances to the TCCC platform are paramount to address future theatre needs.
Disruptive Technologies
Significant improvement in pre-hospital far forward survival rates have been achieved from previous conflicts by continued analysis of injuries and mortalities that has resulted in the refinement of tactical combat care practices. The reduction of Golden Hour en route transport times, use of alternative resuscitation blood products, and changes in tourniquet practices are examples of evolutionary changes that have been implemented and have had a profound impact on survival rates. It is proposed that beginning with a new paradigm for those biomarkers used to recognize a disease condition, there are several disruptive technologies needed to develop an autonomous small form factor medical platform that is envisioned as providing “Trauma Care in a Rucksack”. Each technology proposed (Figure 1) serves as a building block to the next to fully address future theater requirements. The following is a list of proposed disruptive technologies needed to address future dense urban combat casualty theater requirements.
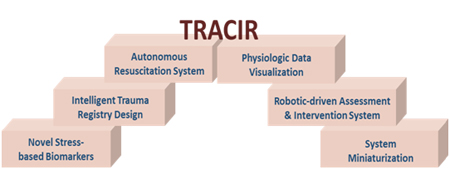
Figure 1: TRACIR's Disruptive Technology Building Blocks
Novel Stress-based Biomarkers
While many improvements to Tactical Combat Casualty Care (TCCC) have been made, advancements in the fundamental practice of battlefield medicine where the use of patient vital signs and symptomatic measures (signs and symptoms) to assess and treat the patient have languished. It is posited that this has been the primary impediment towards improving TCCC. Similar to civilian trauma care, the practice of TCCC relies primarily on training the medic or corpsman in the art of interpreting signs and symptoms that are then applied to a complex poly-trauma protocol to guide interventions. Practicing this “art of care” approach is extremely challenging even in a more controlled domestic emergent care facility without the logistical challenges of tactical field care or evacuation care or the threat of performing care under fire.
It is widely accepted that regardless of how miniaturized and portable, the use of vital sign sensors such as blood pressure and the capture of symptoms such as the pallor of skin or capillary refill, provides poor detection sensitivity offering limited advanced warning to recognize an impending unstable condition. This is because signs and symptoms occur during latter stages of a response to a trauma insult and are more indicative of the degree of compensatory exhaustion. Signs and symptoms also provide limited discriminatory accuracies to enable early recognition of the different causal poly-trauma states that serve as key decision points to determine an optimal intervention from the TCCC guidelines.
A more valuable biomarker reflects an autonomic nervous system (ANS) stress response. This is because the ANS response is a patient-specific measure of how the cardiovascular (CV) system is adapting to varying forms of stress (e.g. cognitive “fight or flight”, physical exertion, environmental such as heat or cold, disease, trauma insults, etc.) in order to remain stable. Stability can be defined as the ability to constantly adapt circulatory flow to stress related changes in blood flow demand in order to maintain adequate oxygen delivery to the tissues and organs. The current use of signs and symptoms reflects latter stage measures for how well the CV system is adapting to the aggregate effects of stress placed upon it. An abnormal sign or symptom measure is evident when CV adaptation is failing. For example, a static blood pressure provides a general range for when the CV adaptive mechanisms to maintain stability from the stress of hemorrhagic shock have been exhausted offering little to no advanced warning for when to act nor any discriminatory value as to cause.
Alternatively, it is possible to capture non-invasive hemodynamic and metabolic biomarkers that correlate with the various CV adaptive mechanisms themselves that provide an early stage, patient-specific means to characterize a specific stress response. For example, a primary adaptive response to stress is small artery vascular constriction which causes the transfer of blood to flow to the central circuit. [6] [7] This constriction response is activated by a drop in aortic (baroreceptor detected) pressure that enables recognition of increased circulatory flow demand that may have been triggered by the circulatory stress from hemorrhage, exercise or other causes. Activation of small artery vasoconstriction occurs prior to when changes in vital signs and symptoms become evident. Use of a measure of small artery vasoconstriction can serve as a broad event indicator to recognize an impending unstable CV condition and provide an adequate interventional time window to act prior to when the patient decompensates.
Further, if multiple CV adaptive mechanisms (or correlates) inclusive of both hemodynamic and metabolic measures are captured, a more precise characterization of the type of stress response can be captured. Use of machine learning methods can be applied to identify combinations of these novel temporal pattern-based biomarkers with the most predictive accuracy to recognize a specific form of poly-trauma stress response in the future. Further, these poly-stress responses can be translated into software rule-based events similar to how computers continually monitor data streams for software viruses. The use of a poly-trauma event (PT) provides a more precise characterization of the patient’s physiologic states that can serve as the primary building block needed to build an intelligent TCCC platform.
Intelligent Trauma Registries
Registries are currently used for “strategic” medical purposes to enable determination of optimal practices that provide the best outcomes as opposed to having tactical utility. The Office of the Secretary of Defense/Health Affairs directed the services to implement the “Joint Theater Trauma Registry” (JTTR) in December 2004, and more recently evolved into the DoD Trauma Registry (DODTR). The DODTR has had a major impact in documenting the types of wounds and treatments rendered, resulting in clinical process improvements and standardization of provider practice for hospital care. However, still lacking is a comprehensive and integrated system for data collection and analysis to improve performance at the pre-hospital level of care. Capture of the TCCC based casualty cards, after action reports, and unit-based pre-hospital trauma registries, linked with novel sensor biomarkers need to be implemented globally and linked to the DoD Trauma Registry in a seamless manner that will optimize pre-hospital trauma care delivery. [8]
A future value of the data registry is to capture more granular medical data to determine the optimal protocol to perform for a specific poly-trauma event. This could be called an “Intelligent Registry” where the product is a catalog for event-driven, goal-directed care using “operationalized” medical data (captured from point of injury to Role 3 medical facilities) across the evacuation continuum and added to the JTTR. Such an “Intelligent Registry” would not only include the current critical care data elements (i.e. vital signs, treatments rendered) but also include novel biomarkers (i.e. arterial vasoconstriction measurements) in a robust data set leading over time with machine learning to predictive analytics and improved clinical outcomes.
The first data requirement is the need to capture “context” that includes data to describe the patient type. This includes demographics and current physiological state of the casualty to further classify the patient. This is another aspect of the “art of care” that many take for granted, where a clinician typically assimilates information such as ambient temperature and patient age for example, that may be a means to discriminate PT events from one another. This form of medical data can be acquired physiologically or from a medical record such as one stored on a barcode worn by the patient.
The next type of medical data required are those interventions that have been performed on the patient. In an OR setting, the anesthesiologist factors in the type of anesthetics used for example, to anticipate decreases in blood pressure due to known vasodilatory effects from the anesthetic used. Without determining whether the current PT event is resultant of a pharmacological intervention for example, it may be difficult to predict how a patient will respond to additional interventions. This suggests that some cataloged PT events are poly-trauma stress responses in combination with a pharmacologic, blood product or other physiology altering prophylactic. This also implies that there must be some kind of methodology to automate the documentation of interventions employed. In an automated scenario, this becomes much simpler as every intervention is performed by the TCCC device platform and can therefore be recorded. Ultimately a taxonomy of PT events can be developed.
Another important component of the “Intelligent Data Registry” is the knowledge-building aspect of the registry that focuses on building a predictive capability for the efficacy of an intervention performed on a specific patient type exhibiting a specific PT event. This requires performing an ongoing retrospective analysis to evaluate or “score” which interventional protocol has the optimal near-term response and longer-term outcome. Development and sharing of civilian trauma registries with DoD operational medical data registries will accelerate the critical mass of evidence-based medical data needed to more rapidly refine the discriminatory accuracy of PT events to achieve optimal interventional strategies.
Semi-autonomous and Autonomous Resuscitation
Once an intelligent trauma registry structure has been created to capture PT events, formalization of the pathophysiological progression of different types and combinations of trauma insults can be documented. This offers the potential to construct models beginning with animal trauma studies that allow for identification of quantifiable detection thresholds and intervention endpoints that can be further refined with ongoing human registry data collection.
This evidence-based intelligent trauma registry content can, in turn be used to construct an intelligent advisor to guide the corpsman or medic. Alternatively, an autonomous or closed-loop resuscitative capability can be developed. Interventions and key data inflection points can be translated into upper and lower control limits for a servo-driven infusion pump or respirator resuscitation system. Current closed-loop designs provide generalized algorithms with broad utility across many patient types and underlying trauma etiologies. Autonomous systems that have the benefit of ongoing learning from Intelligent Trauma Registry access will be able to continuously refine the evidence-based protocols employed that will ultimately result in improved outcomes and strategies to address outliers not currently possible.
Physiologic Data Visualization
Newer physiologic monitoring device interfaces have a dashboard-like appearance that allow the user to quickly determine whether the physiology parameters collected are within the acceptable ranges per the current standard of care. Current military training relies on visualization of the stop light analogy – i.e. green, yellow, and red indices - reflective of safe, indeterminate or danger zones, respectively. Future user interfaces will appear more like a multi-dimensional 3-D contour plot to reflect the operating ranges for each compensatory mechanism (Figure 2). A prominent bounded operating range will be constructed from evidence-based upper and lower operating control limits for each compensatory dimension contributing to patient stability. By providing a multi-dimensional process control-like visual, it will be intuitive when patient stability is beginning to head outside of optimal operating range and which compensatory contribution requires intervention - a minor or major adjustment. Data visualization tools constructed in this way will also provide more informative remote patient monitoring data to empower telemedicine resources or facilitate improved patient hand-over through the en route care continuum.
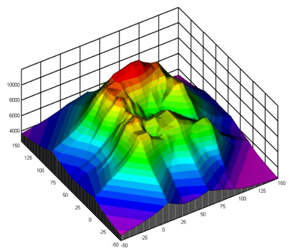
Figure 2: A Visual of a Multi-dimension Contour Plot
Robotic-Driven Assessment & Intervention
An autonomous system must be capable of performing a more comprehensive patient assessment and initiate cardio-pulmonary resuscitation related interventions to support prolonged field care for durations of up to two-hours [5]. Lightweight, highly accurate robotics such as in the form of a “soft” robotics body-wrap will be required to manipulate both the patient and embedded visual arrays with imaging devices to provide a more complete assessment of the patient. Likewise, image-guided robotic strategies can be employed to identify those physiologic landmarks to perform image-guided needle placement to facilitate ventilatory (cricothyrotomy or thoracostomy) or circulatory (endovascular aortic balloon placement for non-compressible hemorrhage) interventions. These capabilities are perhaps the most “DARPA-hard” of the disruptive technologies mentioned. More extensive discussions are required to accommodate all possible use cases and logistical challenges to fully assess the requirements for this type of capability.
System Miniaturization
Common to all technologies discussed, a primary consideration must be given to size and weight requirements that enable accommodating a “rucksack” form-factor. Given the advances made in integrated sensor design, mobile platform computational capabilities capable of rapid local signal processing, integrated communications, and nominal power requirements, miniaturization is perhaps more evolutionary rather than revolutionary and disruptive. However, the clinical utility afforded by a portable ICU quality TCCC platform that can be easily transported to the point-of-injury is indeed disruptive.
Conclusion
The “Trauma Care in a Rucksack” (TRACIR) concept addresses many of the combat casualty care operational deficiencies identified in past conflicts by proposing a novel approach to a fundamental technical challenge. This challenge is to overcome the pervasive use of subjective physiologic signs and symptoms used as the standard of care to triage or assess and treat patients that is also an obstacle towards providing a semi-autonomous and autonomous Tactical Combat Casualty Care (TCCC) solution. A set of disruptive technology building blocks is proposed to create a paradigm shift in how medical data is defined, stored, captured, visualized, and shared such that a more easily transportable semi-autonomous and autonomous TCCC solution can be developed. The proposed TRACIR platform satisfies key operational requirements for use by any vehicle of opportunity, during prolonged field care in denied environments, and for future Unmanned Aerial Systems’ needs.
References
- Thomas B, Amouzegar MA, Costello R, Guffey RA, Karode A, Lynch C, Lynch KF, Munson K, Ohlandt CJR, Romano DM, Sanchez R, Tripp RS, Vesely JV. Project AIR FORCE Modeling Capabilities for Support of Combat Operations in Denied Environments. http://www.rand.org/content/dam/rand/pubs/research_reports/RR400/RR427/RAND_RR427.pdf; accessed 11 February 2016.
- U.S. Army Roadmap for UAS 2010-2035.http://www-rucker.army.mil/usaace/uas/us%20army%20uas%20roadmap%202010%202035.pdf; accessed 11 February 2016.
- Force 2025 and Beyond: Preparing to Win in a Complex World. http://www.arcic.army.mil/Articles/f2025bd-Force-2025-and-Beyond-Preparing-To-Win-In-A-Complex-World.aspx; accessed 11 February 2016.
- Meystel AM, Albus JS; Intelligent Systems Architecture, Design, and Control; John Wiley & Sons, Inc. 2002; page 3.
- Combat Trauma Lessons Learned from Military Ops of 2001-2013.Defense Health Board, Office of Assistant Secretary of Defense; Health Affairs; March 2015.
- Hall, John. Textbook of Medical Physiology. (12th ed.). Elsevier Science Publishers. p. 184. ISBN 9788480868198.
- Klaubunde, Richard. Cardiovascular physiology concepts. (2nd ed.). Lippincott Williams & Wilkins. p. 181. ISBN 9781451113846.
- Kotwal RS, Butler FK, Montgomery HR, Brunstetter TJ, Diaz GY, Kirkpatrick JW, Summers NL, Shackelford SA, Holcomb JB, Bailey JA. The Tactical Combat Casualty Care Casualty Card TCCC Guidelines - Proposed Change 1301. J Spec Oper Med. 2013 Summer;13(2):82-7.